Author: Munir Karjaghli, Clinical Applications Specialist, Hamilton Medical AG
Date of first publication: 15.11.2021
Mechanical ventilation during one‑lung ventilation (OLV), also known as single‑lung ventilation, has three goals: (I) to aid in carbon dioxide elimination, (II) to maintain oxygenation, and (III) to reduce postoperative lung dysfunction. Numerous studies have been conducted to determine the most appropriate strategy for mechanical ventilation during OLV.
Many different factors can contribute to perioperative ALI. Lung injury results from mechanical stress caused by hyperinflation, hyperperfusion, and cyclic recruitment/de‑recruitment, together with proinflammatory or biochemical factors. In the case of thoracic surgery patients, a ‘multiple‑hit' theory suggests that a combination of surgery‑related factors, one‑lung ventilation, underlying diseases and co‑morbidities, prior therapy, and other unidentified events may result in greater susceptibility to ALI (
One‑lung ventilation during and after thoracic surgery increases the risk of volutrauma, barotrauma, atelectrauma, and oxygen toxicity, all of which are serious complications that cause ventilator‑induced lung injury (
There is very little data that specifically supports a particular approach to management of OLV in terms of clinical outcomes. The definition of what is considered protective OLV is mainly influenced by expert opinion, evidence gathered from two‑lung ventilation in general surgical patients, and a small number of clinical trials. It is very difficult to pinpoint tidal volume, for example, as a single factor contributing to lung injury during OLV. No study to date has definitively demonstrated any specific advantage of low tidal volume (VT) ventilation during OLV in the absence of other ventilatory strategies, such as positive end‑expiratory pressure (PEEP) (
A retrospective study conducted after implementing a protective ventilation protocol during OLV for lung cancer surgery, which included reduced VT, increased PEEP, limited ventilator pressures, and recruitment maneuvers, found a lower risk of acute lung injury (
The Society for Translational Medicine presents recommendations based on the current evidence for one‑lung ventilation in their Clinical Practice Guidelines for mechanical ventilation management for patients undergoing lobectomy (
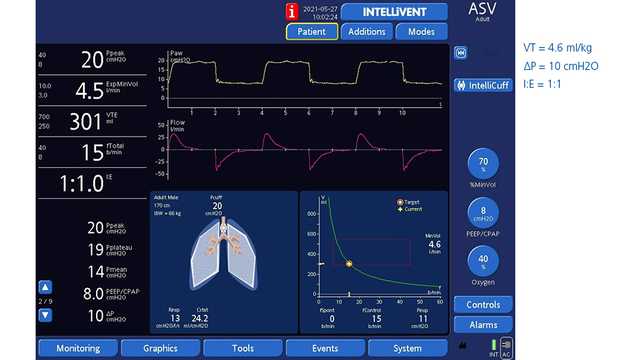
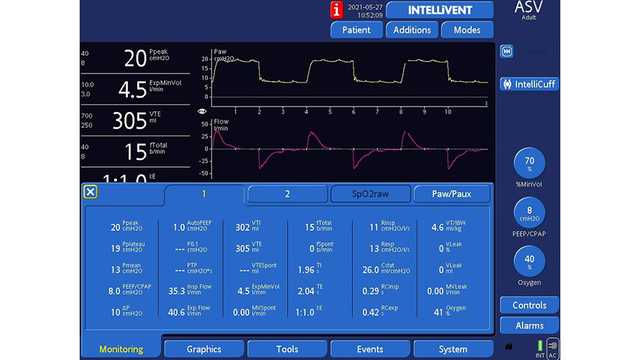
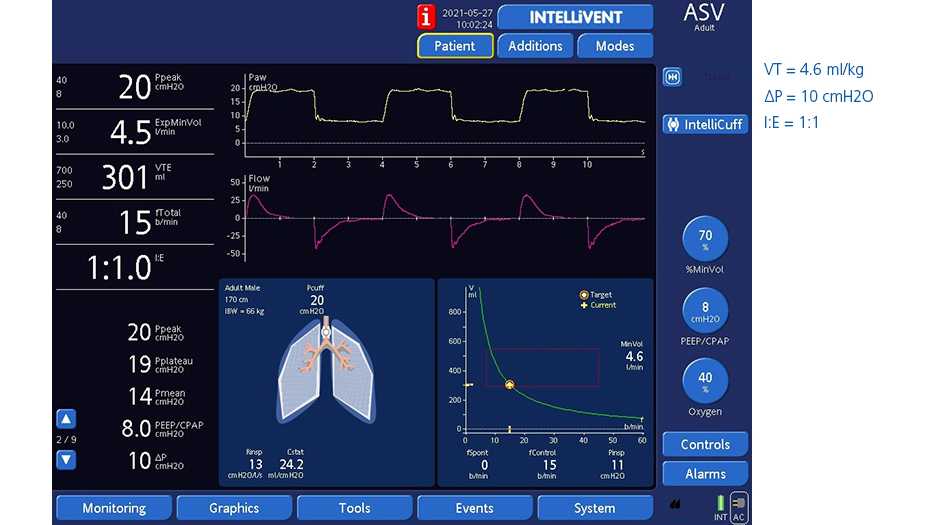
The Adapative Support Ventilation® (ASV®) mode on all Hamilton Medical ventilators automatically implements a lung‑protective strategy compliant with tidal volume recommendations and driving pressure in OLV. Additionally, the fully closed‑loop mode INTELLiVENT®‑ASV (
A study from Weiler et al. shows that ASV can ventilate patients safely, even under the highly variable conditions of OLV (
Figures 1 and 2 below show a 61‑year‑old male patient who underwent a right pneumonectomy being ventilated in ASV.
Full citations below: (