Warum unterscheidet sich der aktuelle Loop für das volumetrische Kapnogramm vom Referenz‑Loop?
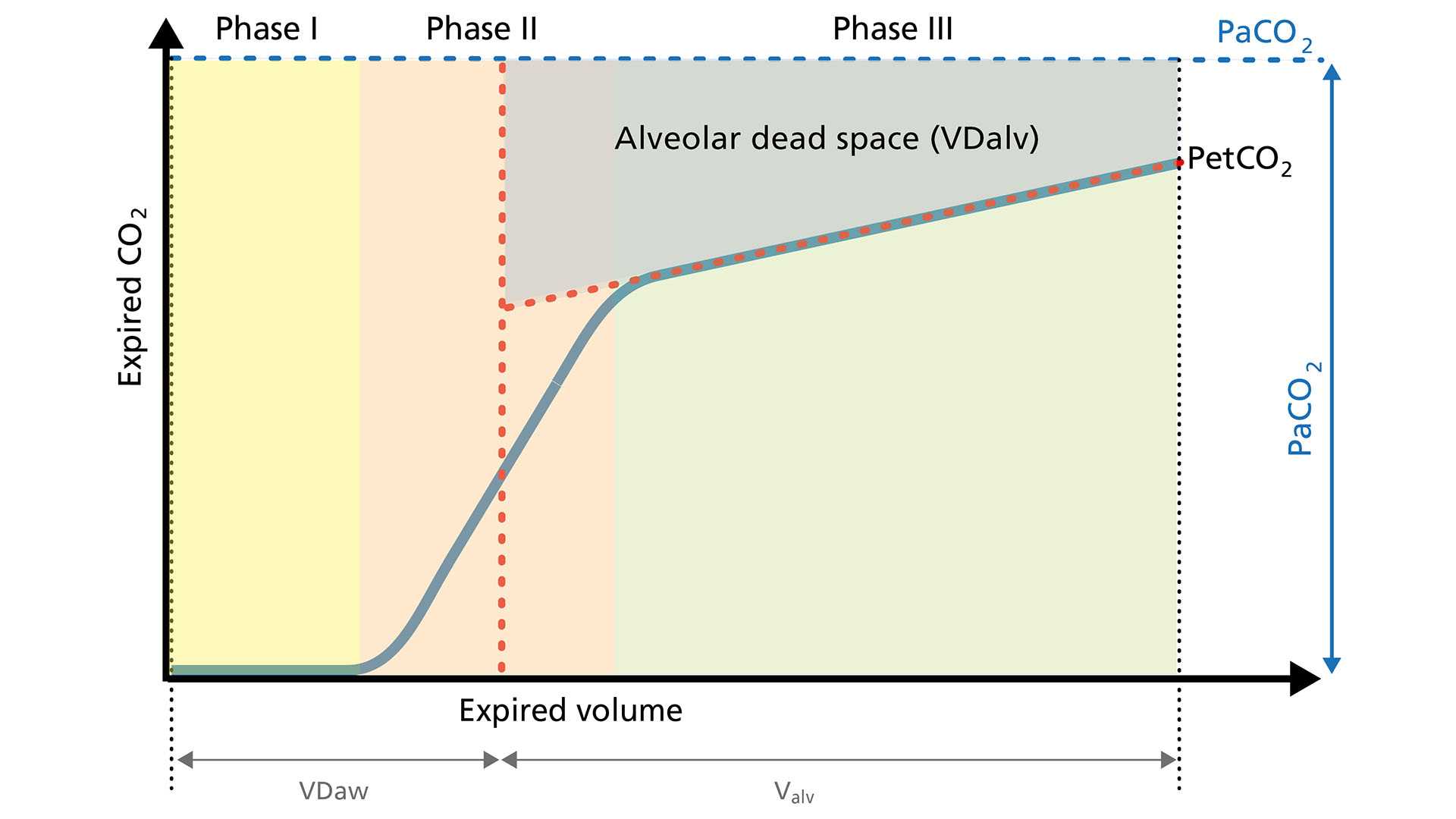
Lungenembolie (LE). Bei einer Lungenembolie ist der alveoläre Totraum (VDalv) durch den verringerten Blutfluss in die gut belüfteten Alveolen erhöht. Dieses Gas mit niedrigem CO2‑Gehalt wird synchron mit dem Gas aus normal perfundierten Alveolen ausgeatmet. Darin unterscheidet sich die LE von Lungenerkrankungen, die den Atemweg betreffen und die durch eine asynchrone Entleerung der Lungenkompartimente mit einem ungleichmäßigen Ventilations‑Perfusions‑Verhältnis gekennzeichnet sind (

Mit dem Anstieg von VDalv nimmt der CO2‑Gehalt im ausgeatmeten Gas ab, was in weiterer Folge zu einem Abfallen des VCO2‑Wertes führt. Der Loop für das volumetrische Kapnogramm ist durch einen deutlich niedrigeren PetCO2‑Wert und ein flacheres Plateau in Phase III gekennzeichnet. Außerdem ist der Anstieg in Phase II weniger steil.