Autor: Jean‑Pierre Revelly, Giorgio Iotti
Datum: 03.04.2023
In diesem Artikel werden die verschiedenen Komponenten der Mechanical Power, ihre Bedeutung in einer klinischen Situation und ihre Verwendung als Monitoring‑Parameter beleuchtet.
Diese Betrachtung beschränkt sich auf die Mechanical Power (MP) während der Inspirationsphase der kontrollierten Beatmung unter der Annahme, dass es keine Atembemühungen seitens des Patienten gibt.
Aus der Physik:
Bei der maschinellen Beatmung ist die während der Inspiration vom Beatmungsgerät auf das Atemsystem übertrage Leistung eine übergeordnete Variable, in der die verschiedenen Elemente kombiniert sind, die eine beatmungsinduzierte Lungenschädigung (VILI) hervorrufen können (
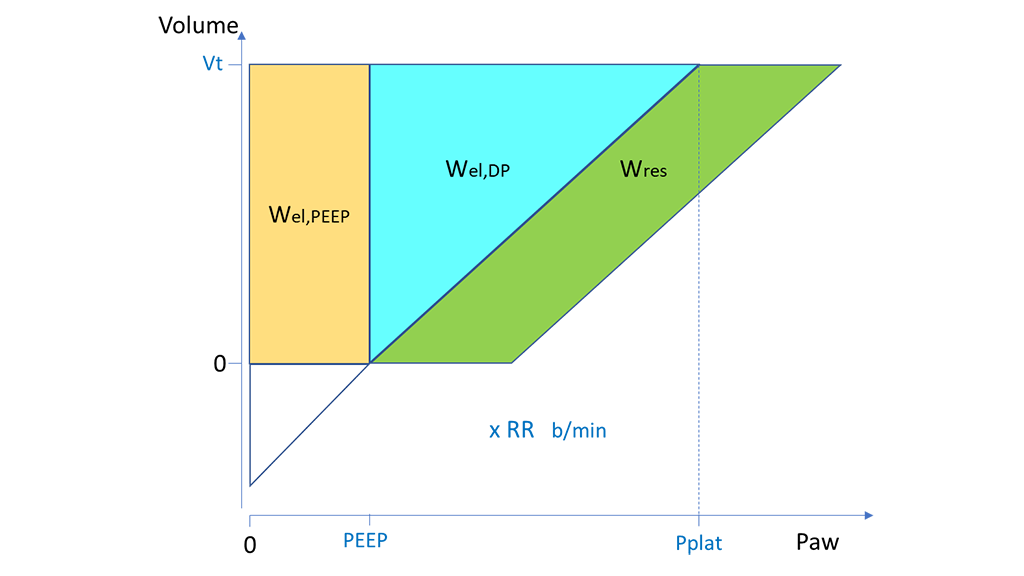
Bei der kontrollierten mandatorischen Beatmung (CMV) mit konstantem Flow kann MP ausgedrückt werden als Arbeit pro Atemhub (W) mal Atemfrequenz (AF) (Abbildung 1) (
Wobei gilt:

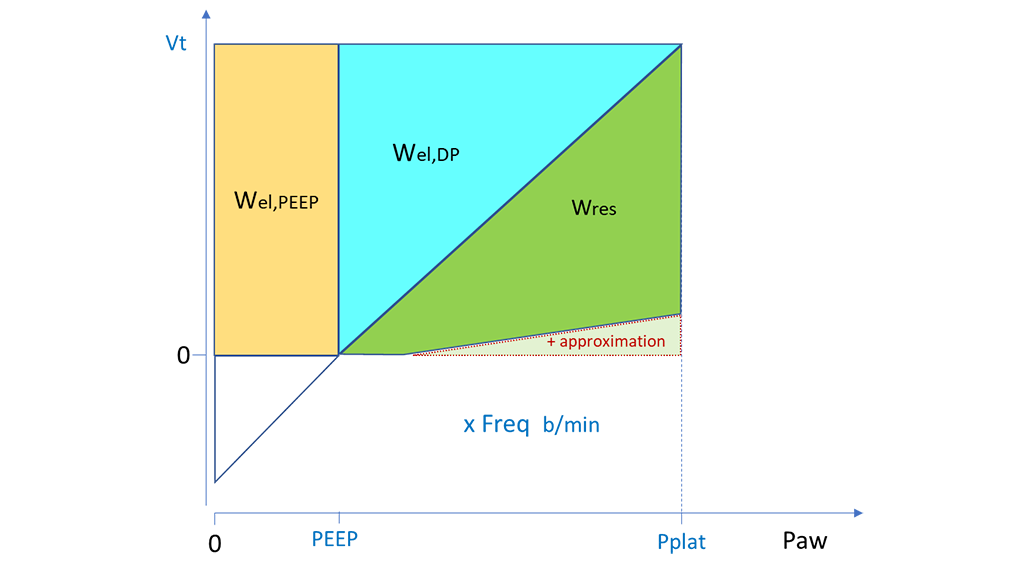
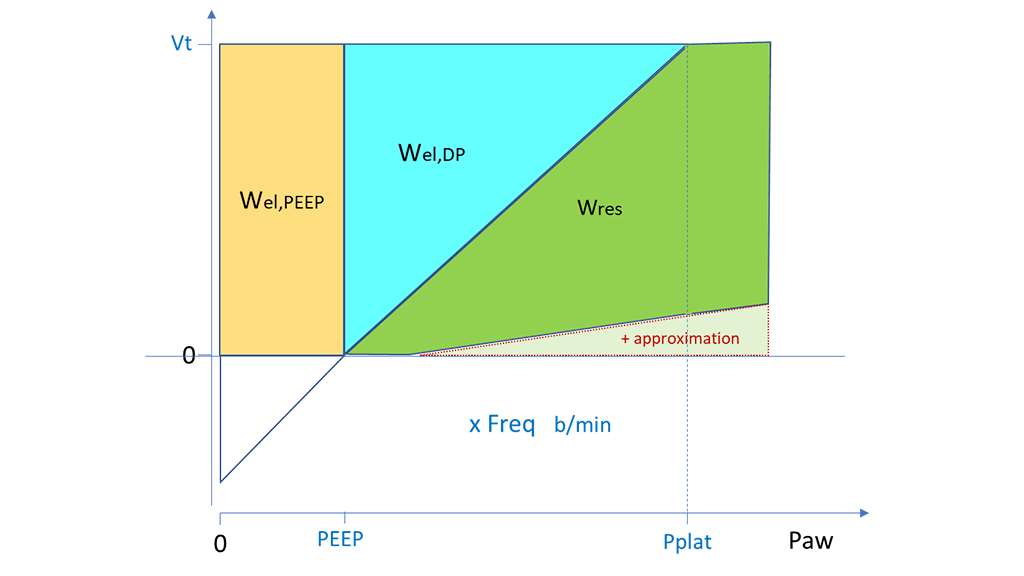
Ein ähnlicher Ansatz kann bei der druckkontrollierten Beatmung (PCV) für die Berechnung von Wel,PEEP und Wel,DP basierend auf Vt, PEEP und DP angewandt werden. Ein Näherungswert für Wres kann berechnet werden, indem die Fläche des Dreiecks mit Ppeak minus PEEP als Basis und Vt als Höhe errechnet und dann das Dreieck für Wel,DP abgezogen wird. Dieselbe Berechnung von Wres kann auch herangezogen werden, wenn Ppeak identisch mit Pplat ist (Abbildung 2) oder höher liegt (Abbildung 3), also wenn der endinspiratorische Flow null bzw. noch positiv ist. In beiden Fällen führt der Näherungswert zu einer leichten Überbewertung von Wres und somit der echten Gesamtarbeit des Beatmungsgerätes (


Zahlreiche Studienärzte haben Mechanical Power aus den Daten verschiedener Beatmungsstudien an Intensivpatienten mit (
Ergebnisse dieser Analysen:
Diese retrospektiven Studien legen insgesamt nahe, dass eine zu hohe Mechanical Power nach Möglichkeit vermieden werden sollte. Dieser Schlussfolgerung liegt die Annahme zugrunde, dass ein schlechteres klinisches Behandlungsergebnis teilweise auf VILI zurückzuführen ist.
Die Methoden, die zur Berechnung der MP in veröffentlichten Studien verwendet wurden, müssen genau betrachtet werden, um eine korrekte Interpretation zu ermöglichen. Je nach Verfügbarkeit der Daten ist es möglich, dass die Autoren diverse Komponenten der MP nicht berücksichtigt haben. Es ist auch umstritten, welche Methode zum Vergleichen der verschiedenen Patienten am besten geeignet ist. Ein Vorschlag umfasst eine Normalisierung der Größe des Patienten (voraussichtliches Körpergewicht), der Compliance oder des endexspiratorischen Lungenvolumens.
Generell ist zu beachten, dass es noch keinen standardisierten Ansatz für die Berechnung der MP gibt. Ebenso wurde kein weithin akzeptierter sicherer Wert für die geschätzte MP definiert.
Individuelle Änderungen an den Einstellungen am Beatmungsgerät haben komplexe Auswirkungen auf andere Variablen der Beatmungsmechanik. Das Konzept der Mechanical Power beruht auf der implizierten Annahme, dass alle Beatmungsvariablen ein lineares Verhältnis zueinander haben und gleichermaßen zur VILI beitragen. Dies trifft jedoch nicht zu, wie am Beispiel von PEEP zu erkennen ist, dessen Verhältnis zur VILI kurvenförmig (J‑Form) ist (
Wenn auch eine Reihe von Fragen unbeantwortet bleibt, dürfte es nützlich sein, die Gesamt‑MP und ihre Komponenten zu überwachen, um die Entwicklung des einzelnen Patienten oder seine Reaktion auf Änderungen in den Beatmungseinstellungen zu bewerten. Die Mechanical Power könnte ein weiterer Faktor neben anderen Komponenten bei der klinischen Bewertung und Entscheidungsfindung werden. Zudem würde die Überwachung der MP das Sammeln hochqualitativer Daten für zukünftige prospektive Studien zum Verhältnis zwischen MP und VILI bedeutend fördern.
Verschiedene Studienärzte haben versucht, die schädlichsten Komponenten der Beatmung zu identifizieren. Eine retrospektive Studie fasste die Beatmungsdaten von 4.500 ARDS‑Patienten, die an kontrollierten Studien teilgenommen hatten, zusammen und beurteilte mit multivariablen Modellen das Verhältnis von MP, Vt, AF und DP zur 28‑Tage‑Sterblichkeit (
Es kommt wenig überraschend, dass die Autoren einen Zusammenhang zwischen der Gesamt‑MP und der Sterblichkeit fanden. Bei der Beurteilung der verschiedenen Komponenten der MP war nur die elastisch‑dynamische Komponente (MPel,DP, also MP in Abhängigkeit von Wel,DP) statistisch relevant; die von PEEP oder der Resistance abhängigen Komponenten waren statistisch nicht relevant. MPel,DP ist bei der CMV‑ wie bei der PCV‑Beatmung besonders einfach am Patientenbett zu ermitteln.
Die Autoren fanden eine ähnliche Prädiktivität der Sterblichkeit, indem sie einfach DP und AF in folgendem Index vereinten:
Die Autoren kamen zu folgendem Schluss: „Wenn auch die Mechanical Power mit der Sterblichkeit bei ARDS‑Patienten in Verbindung stand, so gaben ∆P und AF ebenso viel Aufschluss und konnten am Patientenbett leichter bestimmt werden. Ob eine Beatmungsstrategie auf Basis dieser Variablen das Behandlungsergebnis positiv beeinflusst, muss in randomisierten Studien geprüft werden“ (