Autor: Jean‑Michel Arnal
Datum: 09.04.2024
Eine bewährte Methode zur Beurteilung der Rekrutierbarkeit der Lunge ist die Verwendung einer Druck/Volumen‑Kurve.
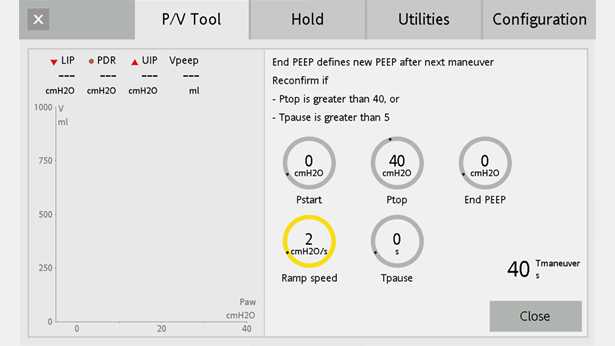
Die Beurteilung der Rekrutierbarkeit am Patientenbett kann bei komplett passiven Patienten mit früh auftretendem ARDS durchgeführt werden, wenn keine Leckagen im Beatmungskreislauf auftreten. Im Tab P/V Tool (
Beachten Sie, dass dieselbe Beurteilung mit den Standardeinstellungen am Beatmungsgerät für P Start und End PEEP (5 cmH2O) durchgeführt werden kann.
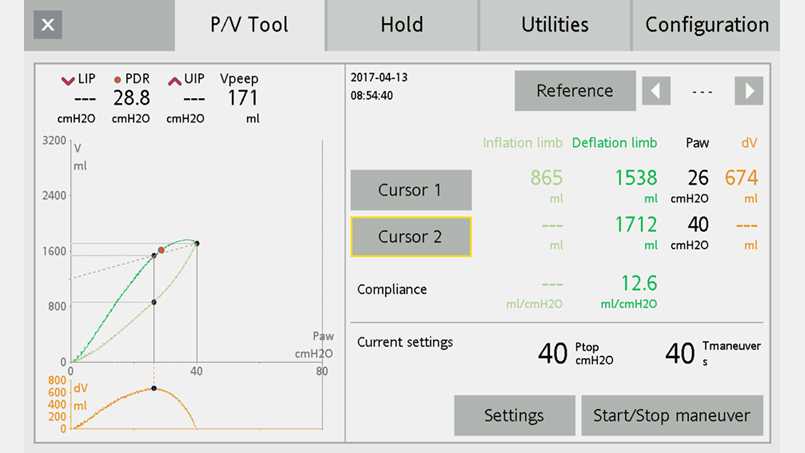
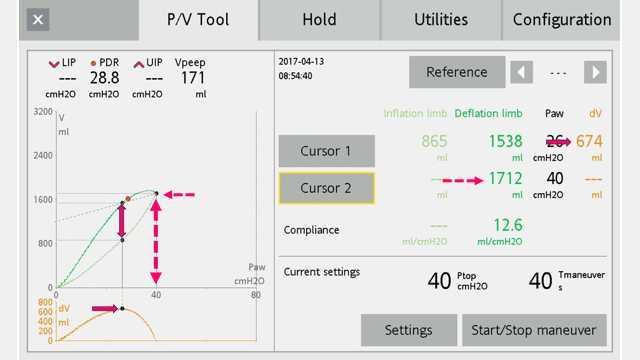
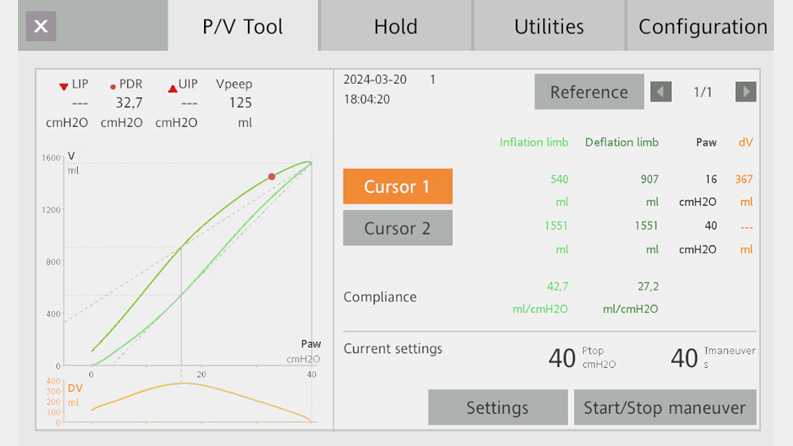
Wählen Sie die Grafik, die die P/V‑Kurve gemeinsam mit der automatischen Berechnung des Volumenunterschieds für jeden Druck darstellt (Paw/V + Paw/dV) (Abbildungen 2 und 3).
Jetzt können Sie den normalisierten Maximalabstand (NMA) berechnen. Der NMA wird in Prozent ausgedrückt und entspricht dem Maximalabstand dividiert durch das Maximalvolumen.
Im vorliegenden Beispiel: NMA = (674/1712) x 100 = 39%
Der Wert für NMA% von 41 kann herangezogen werden, um Lungen mit hohen Erfolgsaussichten für das Recruitment (NMA% ≥ 41) von Lungen mit niedrigen Erfolgsaussichten zu unterscheiden, bei denen sich ein Recruitment als schwieriger erweisen könnte (NMA% < 41) (


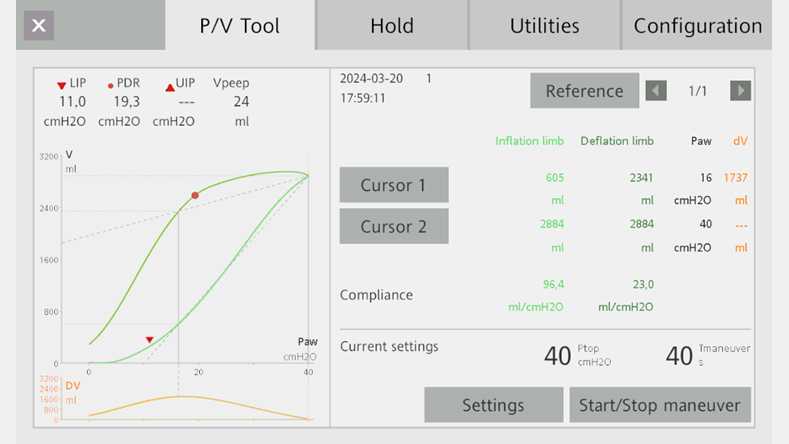
Abbildung 4:
Herr A. ist ein 72‑jähriger Patient, der mit ARDS aufgenommen wurde.
NMA = (1737/2884) x 100 = 60 %
Dieser Patient wird wahrscheinlich von einer Recruitmentstrategie profitieren.
Abbildung 5:
Herr L. ist ein 66‑jähriger Patient, der mit ARDS aufgenommen wurde.
NMA = (367/1551) x 100 = 24 %
Dieser Patient wird wahrscheinlich nicht von einer Recruitmentstrategie profitieren.