
Author: Jean‑Michel Arnal, Senior Intensivist, Ste Musse Hospital, Toulon, France
Date of first publication: 23.04.2019
PEEP is used to keep the lung aerated and prevent lung collapse at the end of expiration. However, PEEP may over‑distend the normally aerated lung and impair lung perfusion. Therefore, any change in PEEP may affect the overall ventilation/perfusion ratio in an unpredictable way.
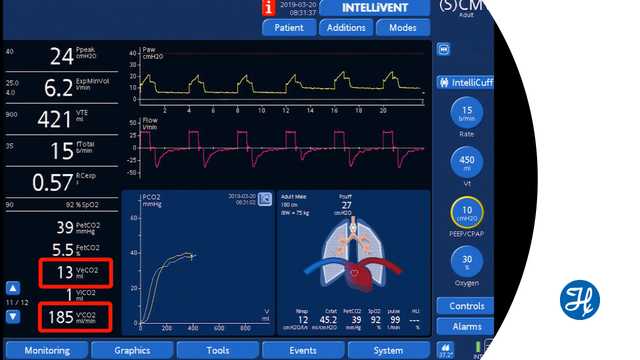
Volumetric capnography measures the volume of CO2 exhaled breath‑by‑breath (VeCO2). After a change in PEEP, assuming that the cardiovascular function and tidal volume are stable, an increase in VeCO2 means that the overall ventilation/perfusion ratio has improved. Conversely, a decrease in VeCO2 means that the ventilation/perfusion ratio is worsening. VeCO2 changes rapidly and returns to the baseline after a few minutes.
The limitation to this method is that the clinician monitors rapid changes to the ventilation/perfusion ratio, such as those due to lung over‑distension and lung‑perfusion impairment or improvement.
After a change in PEEP, recruitment or derecruitment may take a longer time to occur and cannot be assessed by this method.
Watch the video below to see a demonstration during ventilation with a Hamilton Medical ventilator.
Full citations below: (
Learn how to interpret a volumetric capnogram and get an overview of the benefits and clinical applications of volumetric capnography. Includes a self‑test!
