Author: Süha Demirakca
Date of first publication: 12.06.2018
It is very useful for diagnosing the lung condition and its severity in order to optimize the ventilator settings (
This bedside tip provides examples of adjusting settings for pressure, tidal volume (Vt), inspiratory and expiratory time (Ti, Te), and frequency according to the measured airway mechanics (RCexp, C, R) for different lung conditions in children. Note that the flow curve should also be checked in all cases to avoid end-inspiratory and end-expiratory flow interruption. This promotes the best gas distribution during Ti and helps avoid AutoPEEP/air-trapping during Te.
The following images show original monitoring data from mechanically ventilated children.
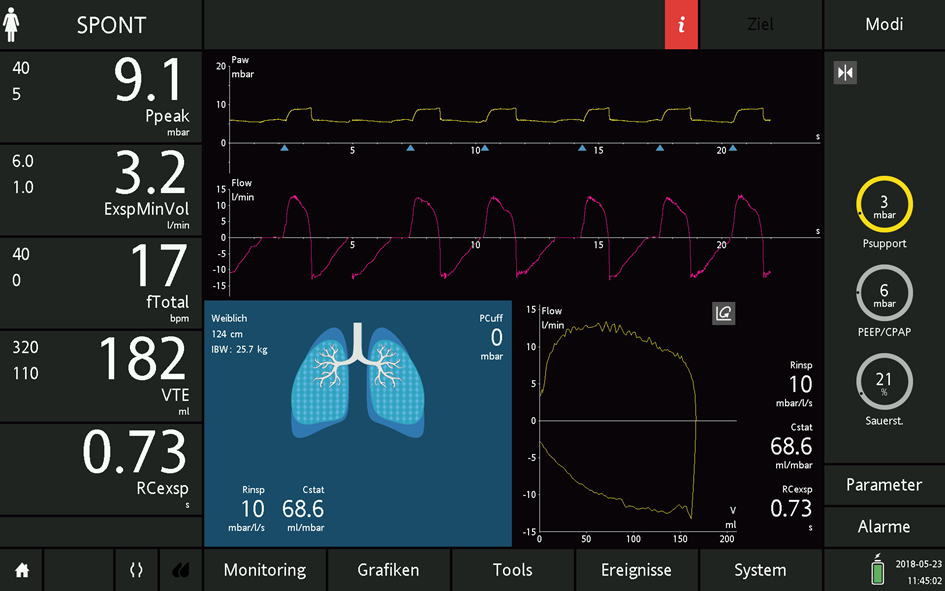
Figure 1 shows a two-year old boy with severe diffuse / interstitial pneumonia under veno-venous ECMO (bodyweight 12 kg). After recovery from self-induced lung injury, sedation was adjusted to limit the respiratory drive. Due to the very low RCexp of 0.10 (C = 2.5 ml/cmH2O; Rinsp = 10 cmH2O/l/s), a protective Pressure support of 9 cmH2O with a resulting Vt of 3.2 ml/kg of bodyweight was chosen. Expiratory trigger sensitivity (ETS) for flow cycling was set to 5% to prevent inspiratory flow interruption occurring too early. Note that the patient compensates the low Vt with a high breathing frequency of 60 bpm, which does not lead to end-expiratory flow interruption.

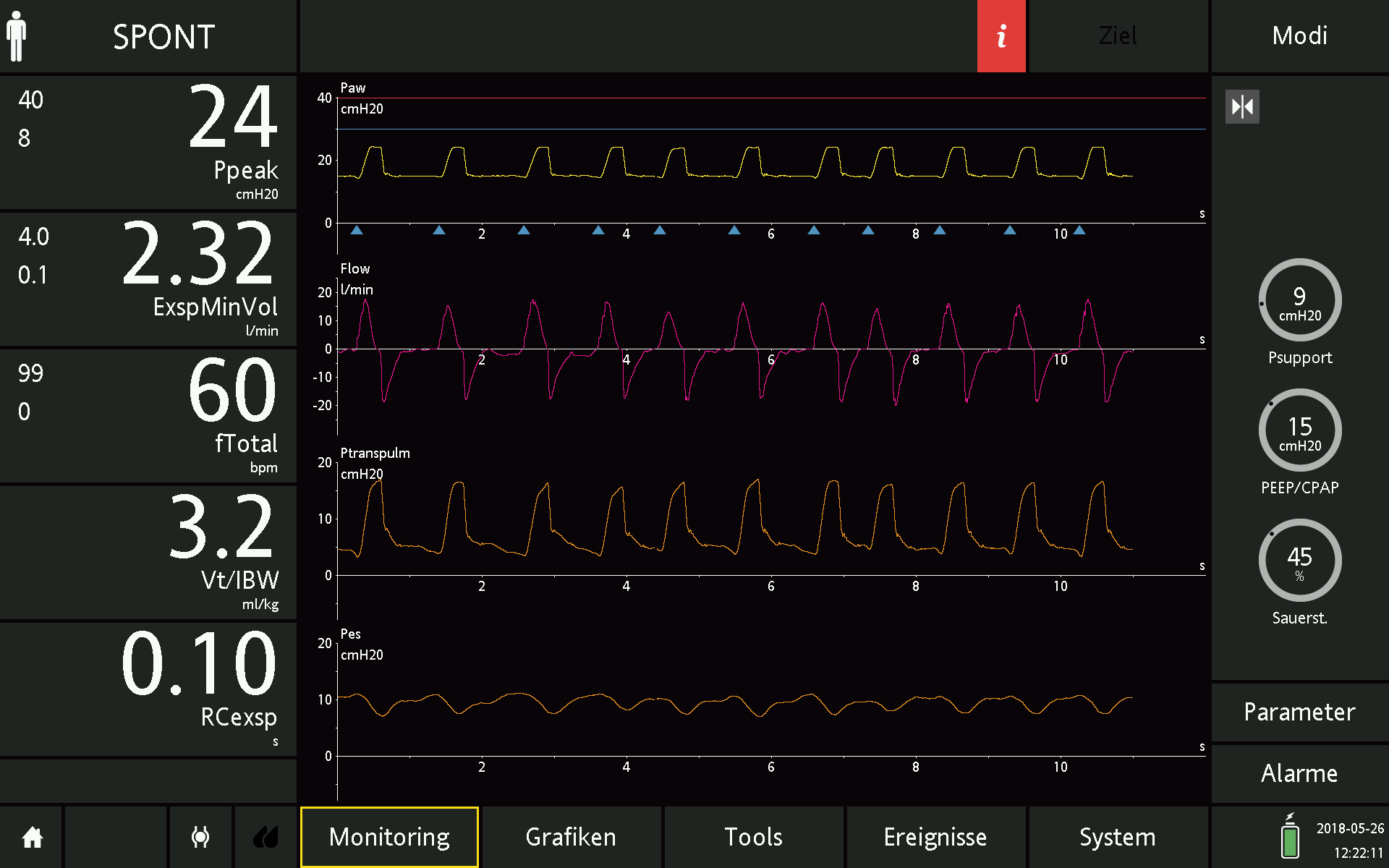
Figure 2 shows a four-year old girl with pneumonia with obstruction (bodyweight 20 kg / length 112 cm) under controlled ventilation. High resistance causes a prolonged RCexp, and the frequency (20 bpm) is lowered with a Ti of 1.1s and Te of 1.9s in order to avoid any flow interruption (see flow curve).

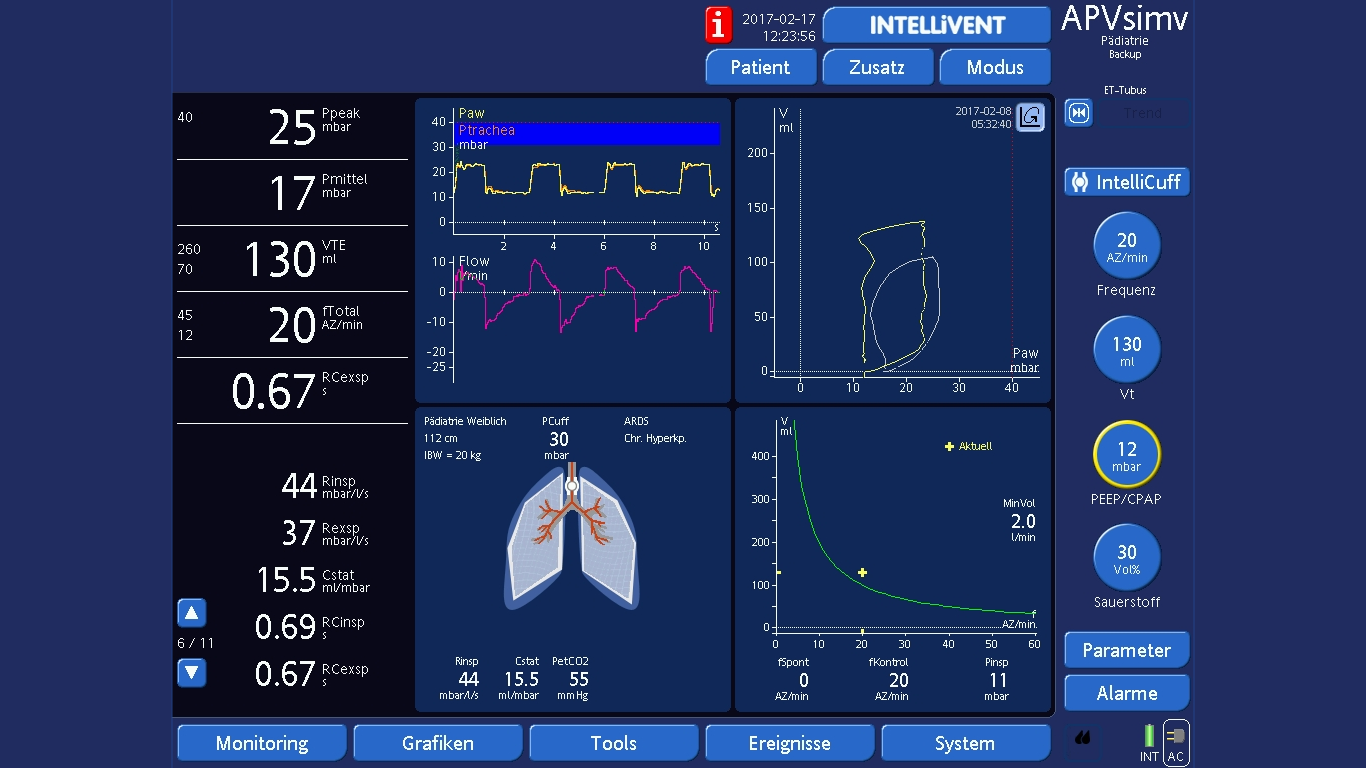
Figure 3 shows an eighteen-month old girl with a BPD history and acute human metapneumovirus pneumonia (bodyweight 9.1 kg) under controlled ventilation. Low frequency (28 bpm) is set together with a protective Vt of 6.6 ml/kg, which is only possible with sedation and permissive hypercapnia (see PetCO2). End-inspiratory and end-expiratory flow interruption is avoided by setting a prolonged Ti and Te.
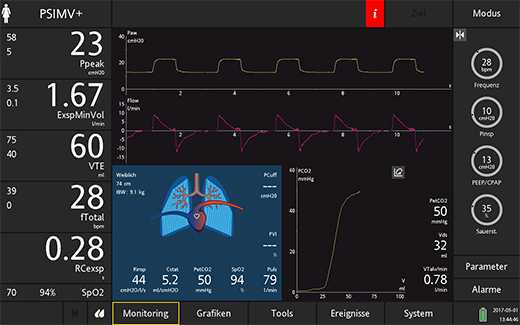
Figure 4 shows a nine-year old girl with neuromuscular disease breathing spontaneously and ready for extubation. Lung mechanics after recovery from pneumonia are normal, with the exception of augmented Cstat due to higher chest wall compliance with reduced muscular tonus (Vt ~7 ml/kg requiring only 3 cm pressure support).