


Author: Jean-Pierre Revelly, Giorgio Iotti
Date of first publication: 03.04.2023
This article takes a closer look at the different components of mechanical power, its relevance in a clinical setting, and its use as a monitoring parameter.
The scope of this discussion is limited to mechanical power (MP) during the inspiratory phase of controlled ventilation, assuming there is no patient effort.
In physics:
In mechanical ventilation, the power transferred from the ventilator to the respiratory system during inspiration is a unifying variable that combines the elements that may cause ventilator-induced lung injury (VILI) (
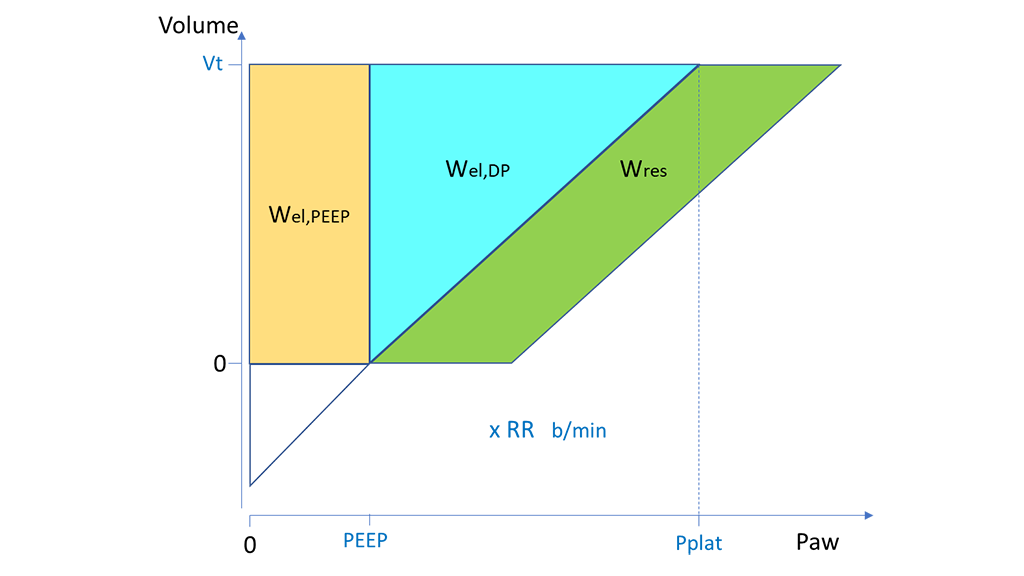
During Controlled Mandatory Ventilation (CMV) with constant flow, MP can be described as work per breath (W) times the respiratory rate (RR) (Figure 1) (
Where:

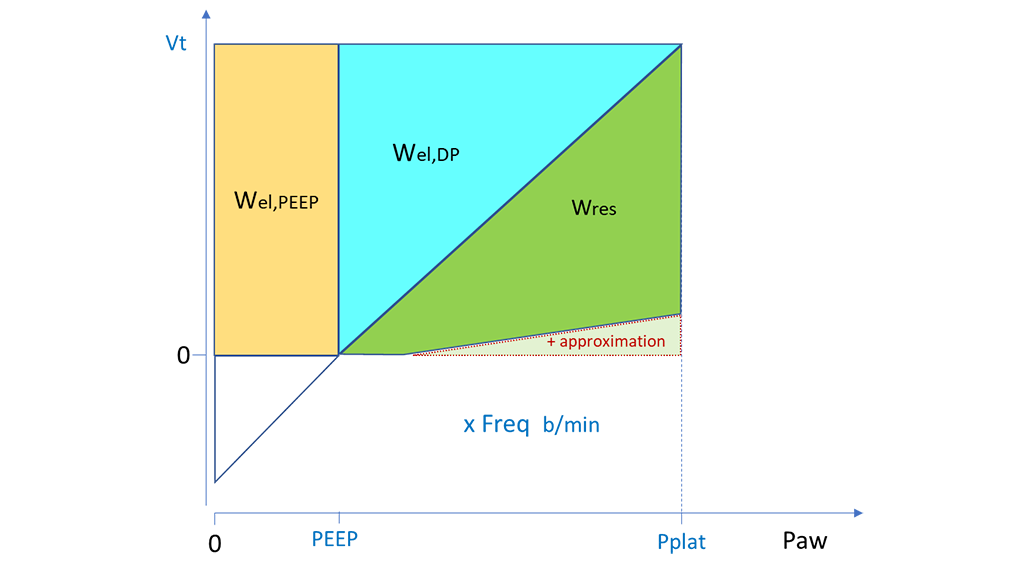
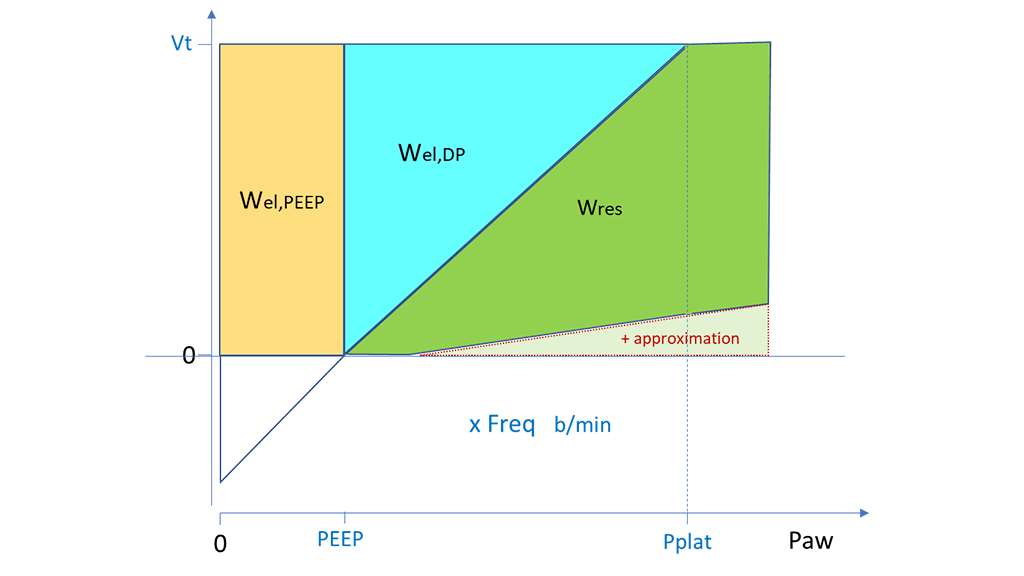
A similar approach can be applied during Pressure Controlled Ventilation (PCV) for the calculation of Wel,PEEP and Wel,DP from Vt, PEEP and DP. Wres can be approximated by calculating the area of the rectangle with Ppeak minus PEEP as base and Vt as height, and then subtracting the triangle corresponding to Wel,DP. This calculation for Wres can be applied in the same way where Ppeak is equal to Pplat (Figure 2) or higher than it (Figure 3), i.e., where the end-inspiratory flow is zero or still positive, respectively. In both cases the approximation results in a slight overestimate of Wres, and hence of the true total ventilator work (


Quite a few investigators have computed the MP from the data of ventilatory studies in ICU patients with (
In these analyses:
Overall, these retrospective studies suggest that excessive MP should preferably be avoided, assuming that a worse clinical outcome was related in part to VILI.
The methods used to calculate MP in published studies must be read carefully to interpret them properly. Depending on the data available, the authors may have included or excluded some of the components of MP. There is also an ongoing debate regarding the most appropriate procedure for comparing different patients. Normalization for the patient’s size (predicted weight), compliance or end-expiratory lung volume have been proposed.
Generally speaking, however, there is not yet a standardized approach for the calculation of MP, nor is there any widely accepted safe value for the estimated MP.
Individual changes of ventilator settings have complex effects on other variables of the ventilation mechanics. The MP concept relies on the implicit assumption that all ventilatory variables have a linear relationship and the same contribution to VILI. However, this is obviously not the case, as PEEP for instance has a curvilinear (J-shape) relationship to VILI (
Although a series of open issues remains, monitoring total MP and its components may prove useful for assessing the individual patient’s evolution or their response to ventilatory setting changes. MP may become a new consideration along with several others in clinical judgement and decision making. Moreover, MP monitoring would greatly help the collection of high-quality data for any prospective study on the relationship between MP and VILI.
Different researchers have tried to identify the most detrimental components of ventilation. A retrospective study compiling the ventilatory data of 4500 ARDS patients enrolled in controlled studies assessed the relationships of MP, Vt, RR and DP to 28-day mortality using multivariable models (
Not surprisingly, the authors found that global MP was correlated with mortality. When assessing the various components of MP, only the elastic dynamic component (MPel,DP, i.e, the MP that depends on Wel,DP) was statistically significant, while the components that depend on PEEP or resistance were not. MPel,DP is particularly simple to calculate at the bedside, in both CMV and PCV.
Moreover, the authors found a similar predictivity of mortality just by combining DP and RR in the following index:
The authors concluded that “although mechanical power was associated with mortality in patients with ARDS, the ∆P and RR were as informative and easier to assess at the beside [sic]. Whether a ventilatory strategy based on these variables improves outcomes needs to be tested in randomized controlled studies” (