
Author: Matthias Himmelstoss
Date of first publication: 02.10.2020
Last change: 14.04.2023
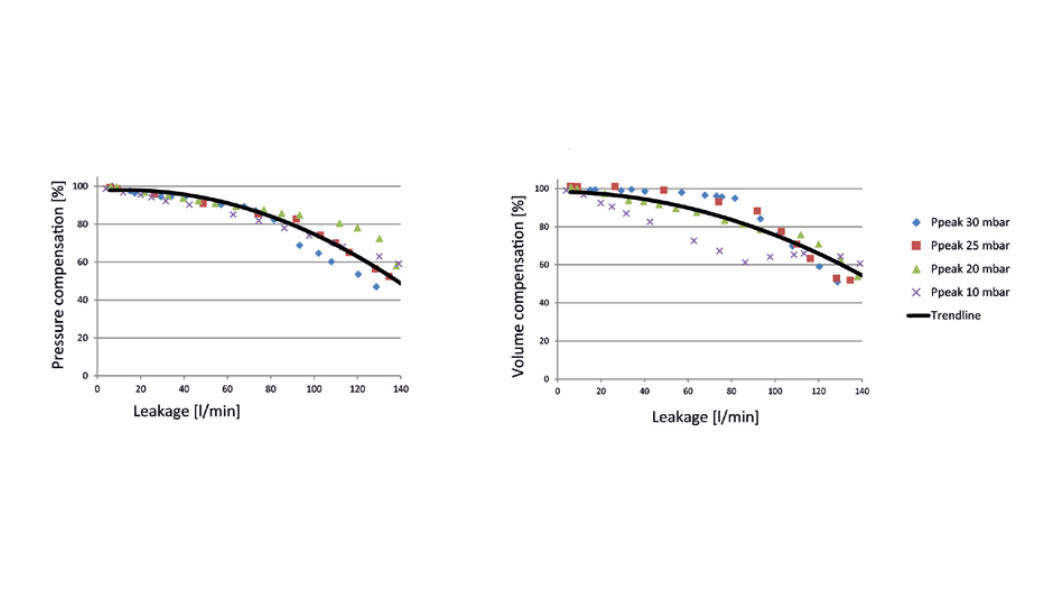
Moved to Public websiteHamilton Medical ventilators provide high leakage compensation during inspiration by assessing the remaining flow at the end of exhalation as an offset for the trigger setting, while maintaining the set PEEP.
We carried out in‑house testing to evaluate maximum airway leakage (simulated mask leak) as the leakage amount where both patient inspiratory and expiratory efforts can still be detected and synchronized to our ventilators without causing auto‑triggering or prolonged exhalation. We made a distinction between the inspiratory leak (leakage present at peak inspiratory flow), where the patient’s expiratory effort is correctly detected by the ventilator, and the expiratory leak (leakage at the end of exhalation), where the patient’s inspiratory effort is still correctly detected by the ventilator and a breath is triggered.
Our results showed that noninvasive ventilation synchronized with spontaneous patient breathing efforts is possible up to the rates shown below.
Relevant devices: HAMILTON‑G5/S1 (SW v2.8x and later); HAMILTON‑C2/C3/C6 (SW v2.2.x and later / SW v2.0.x and later / SW v1.1.x and later; with option IntelliSync+ active); HAMILTON‑C1/T1/MR1 (SW v2.2.x and later)
| HAMILTON‑C6 | HAMILTON‑G5/S1 | HAMILTON‑C2/C3 | HAMILTON‑C1/T1/MR1 | |
| Inspiratory leak compensation | Up to 150 l/min | Up to 75 l/min | Up to 85 l/min | Up to 85 l/min |
| Expiratory leak compensation | Up to 30 l/min | Up to 30 l/min | Up to 30 l/min | Up to 30 l/min |