Author: David Grooms
Date of first publication: 08.07.2019
The frequency of dyssynchronies has been studied and they are estimated to occur at least one time in no less than 50% of patients who receive mechanical ventilation (MV) for more than 24 hours. The two most common dyssynchronies are ineffective (missed) triggering and double triggering (DT) (
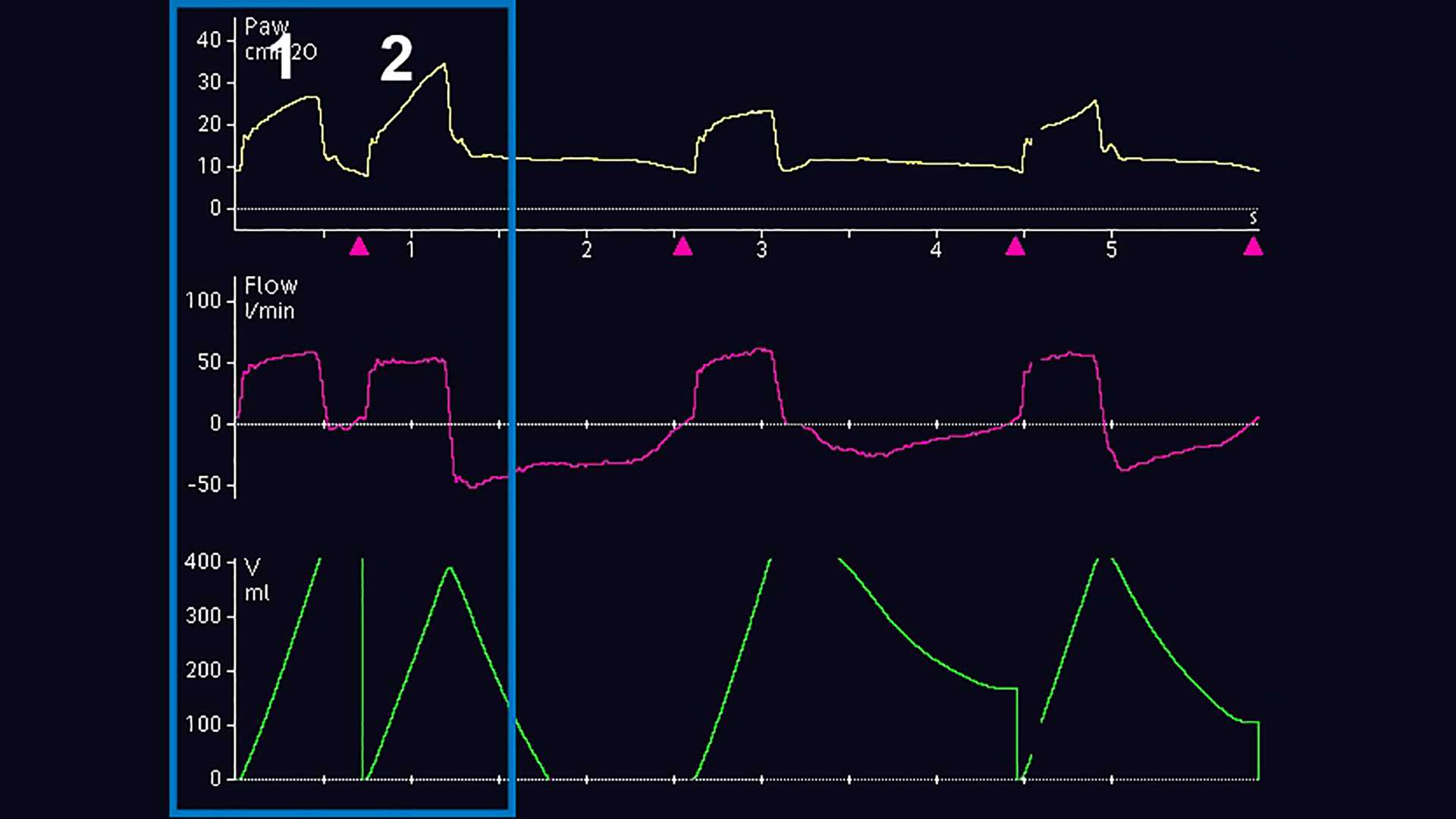
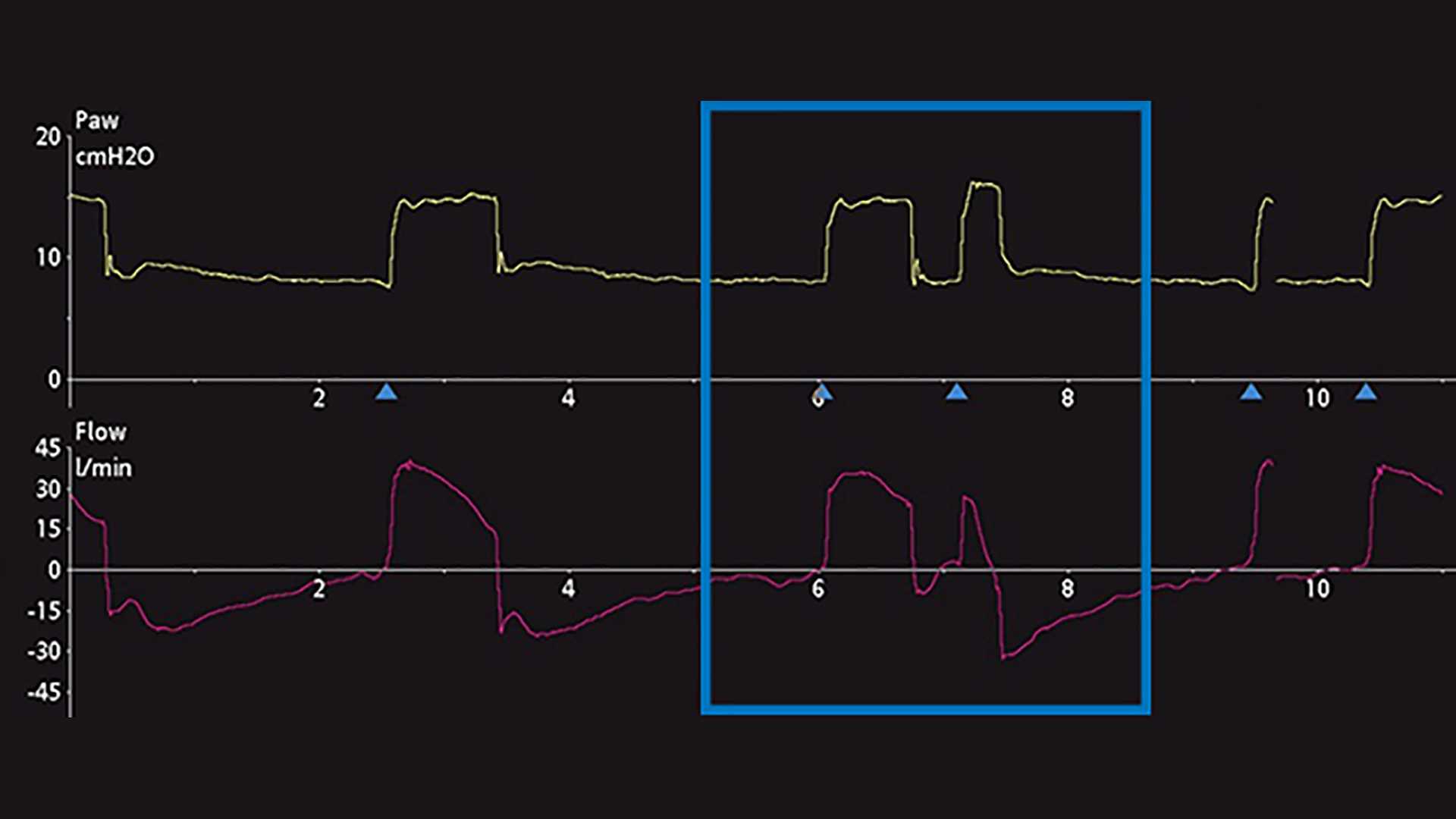
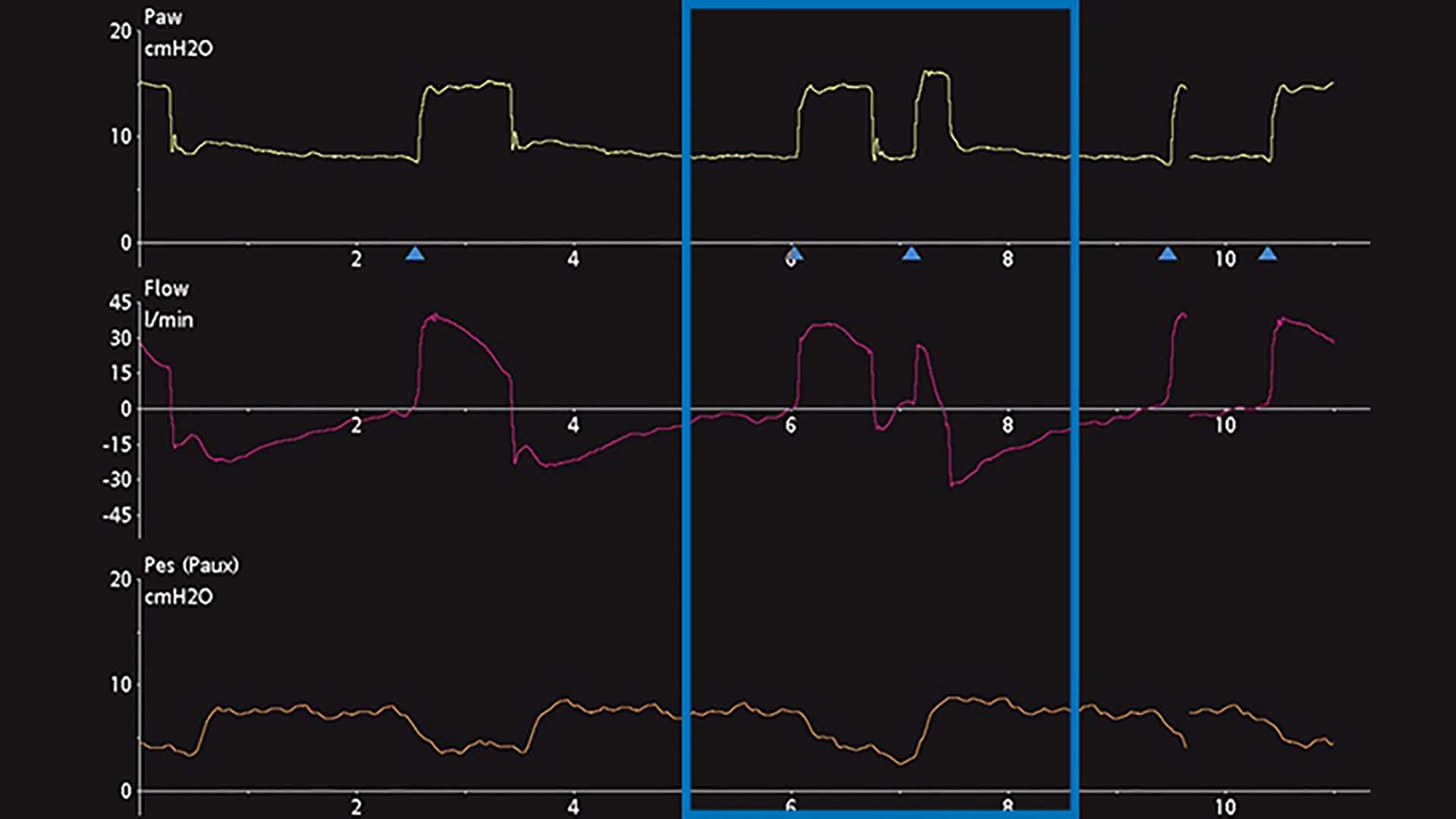
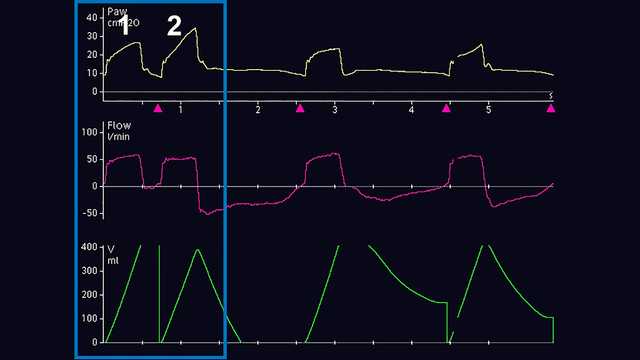
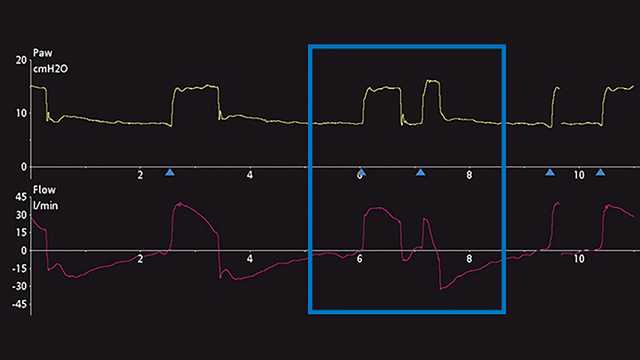
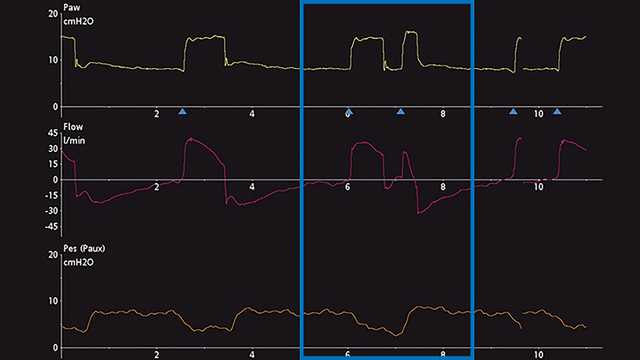
The primary method of DT diagnosis is the observation and evaluation of ventilator scalar waveforms. A scalar waveform is any variable displayed over time. Most mechanical ventilators commonly allow the display of pressure, flow and/or volume over time. To further facilitate the analysis of those waveforms, some ventilators allow the display of esophageal (approximated pleural) pressure over time. To demonstrate the steps toward proper identification of DT, screenshots of ventilator waveforms are provided below. Figure 1 displays common pressure, flow, and volume waveforms revealing the DT phenomenon during invasive ventilation. Initially, the untrained eye may not be able to diagnose this phenomenon, nor may it correctly determine the origin of the problem. Commonly mistaken for the patient actively generating a second breath (Breath 2) after delivery of a mechanically timed breath (Breath 1) or air hunger, this problem can lead to severe adverse effects related to mechanical ventilation if it continues. Therefore, closer analysis is recommended and can be performed by utilizing esophageal manometry to compare and contrast pleural pressure and the ventilator’s airway pressure and flow changes. Another example below, which shows a ventilator displaying pressure and flow time scalars, provides a subtle hint of possible DT, but may also be mistaken for an additional active inspiratory effort (Figure 2). The addition of the esophageal pressure scalar waveform (Pes‑Paux waveform) reveals that in fact a double trigger is present because of the subsequent delivery of breaths during a single active inspiratory effort (see the decrease in pleural pressure in Figure 3).
Differentiating and classifying the type of DT is also challenging at the bedside. Current research suggests that DT can be classified into three different types (
ata has shown there is often a delay in triggering in the pre‑inspiratory phase of between 0.07‑0.13 seconds (
The most common causes for DT are the improper matching of mechanical breath I‑times to neural I‑times, and an insufficient level of pressure support with high respiratory drives (