How is it possible that my patient monitoring system shows a different value for the saturation of peripheral oxygen (SpO2) than the Hamilton Medical ventilator?
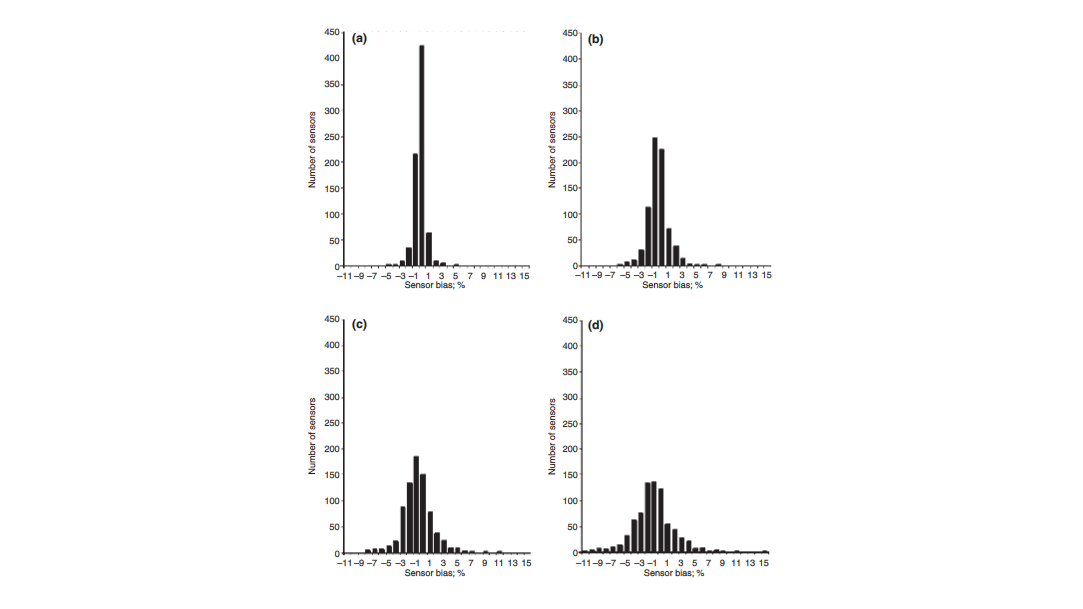
The accuracy of pulse oximetry SpO2 measurements depends on the SpO2 range, patient motion and perfusion. The accuracy of sensors from different manufacturers is typically around ±3% for SpO2 values of > 90% (see Figure 1) (
Therefore, it is possible to have different SpO2 values when using multiple sensors even if using two sensors with the same technology.
If you are using SpO2 measurement in a Hamilton Medical ventilator with the INTELLiVENT®‑ASV® (
If there is a constant difference between the SpO2 and SaO2 values, an SpO2 target shift can be used.
As stated in the INTELLiVENT‑ASV Operator’s Manual, additional ventilator‑independent patient monitoring (for example, bedside vital monitoring or a blood gas analyzer) must be used during ventilation with INTELLiVENT‑ASV.
Relevant devices (for SpO2 measurement option (