

Hamilton Medical offers an optional speaking valve function for the HAMILTON-C1/T1/MR1 ventilators. This function can be activated in the pressure-controlled modes Spont, PCV+ and P-SIMV+.
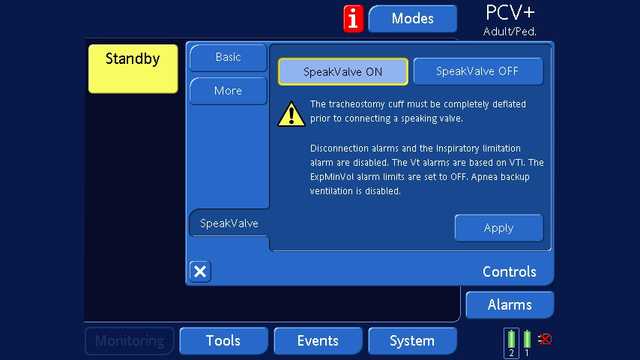
Prerequisites for use of the speaking valve function are sufficient patency (openness) of the upper airways after unblocking the cuff and a speaking valve approved specifically for use with a ventilator e.g. PMV 007 (Aqua Color) (15 mm I.D. / 22 mm O.D.) from Passy Muir. The PMV is basically a one-way valve that only allows air to flow from the ventilator to the patient. As no air can flow back to the ventilator during expiration, all the tidal volume alarms are based on the inspiratory volume when the speaking valve function is in use. The minute volume and apnea alarms are deactivated.
Below you’ll find answers to some common questions about the speaking valve function.
1. Are pressure and volume measured or just calculated? Is it possible to say how much pressure is in the lungs?
Answer: (Inspiratory) pressure and flow are measured at the proximal flow sensor. The extent to which the values displayed (Ppeak, Pmean, PEEP; TI, TE, I:E; VTI) correspond with the pressure in the lungs is the same with a speaking valve as without. However, the ventilator cannot measure expiratory values, as the PMV is closed in the direction of the ventilator and air can only escape via the upper airways.
2. When the patient is talking, the vocal cords open and close. How does the ventilator react to this?
The speaking valve function is only available in pressure-controlled modes. The ventilator therefore tries to reach the set pressure. In the case of leakage, it compensates by already increasing the flow during the breath.
3. Is it to be expected that the alveolar space kept open by PEEP will completely collapse when using a speaking valve?
The evidence has shown that this is not the case. “In this cohort of critically ill ventilated patients, SVs did not cause derecruitment of the lungs when used in the ventilator weaning period. Deflating the tracheostomy cuff and restoring the airflow via the upper airway with a one-way valve may facilitate lung recruitment during and after SV use, as indicated by increased EELI” (
4. Does the pressure support remain as set?
The set Psupport is maintained up to the maximum leak compensation.
5. What is a reliable indicator of airtrapping?
The speaking valve function is only available in pressure-controlled modes and the ventilator therefore tries to reach the set pressure. If the air cannot escape via the upper airways, due to an airway obstruction or accidental inflation of the cuff on the tracheostomy tube, the pressure in the lungs will not increase above the sum of Pcontrol/Psupport and PEEP. In the next breath, the applied inspiratory volume will drop sharply, because the pressure being targeted is already present in the lungs. Therefore, a drop in the inspiratory tidal volume (VTI) is a reliable indicator of situations where airtrapping is starting. As tidal volume alarms are based on inspiratory volumes in the speaking valve mode, this will be recognized.