Auteur: Munir Karjaghli
Date: 09.04.2020
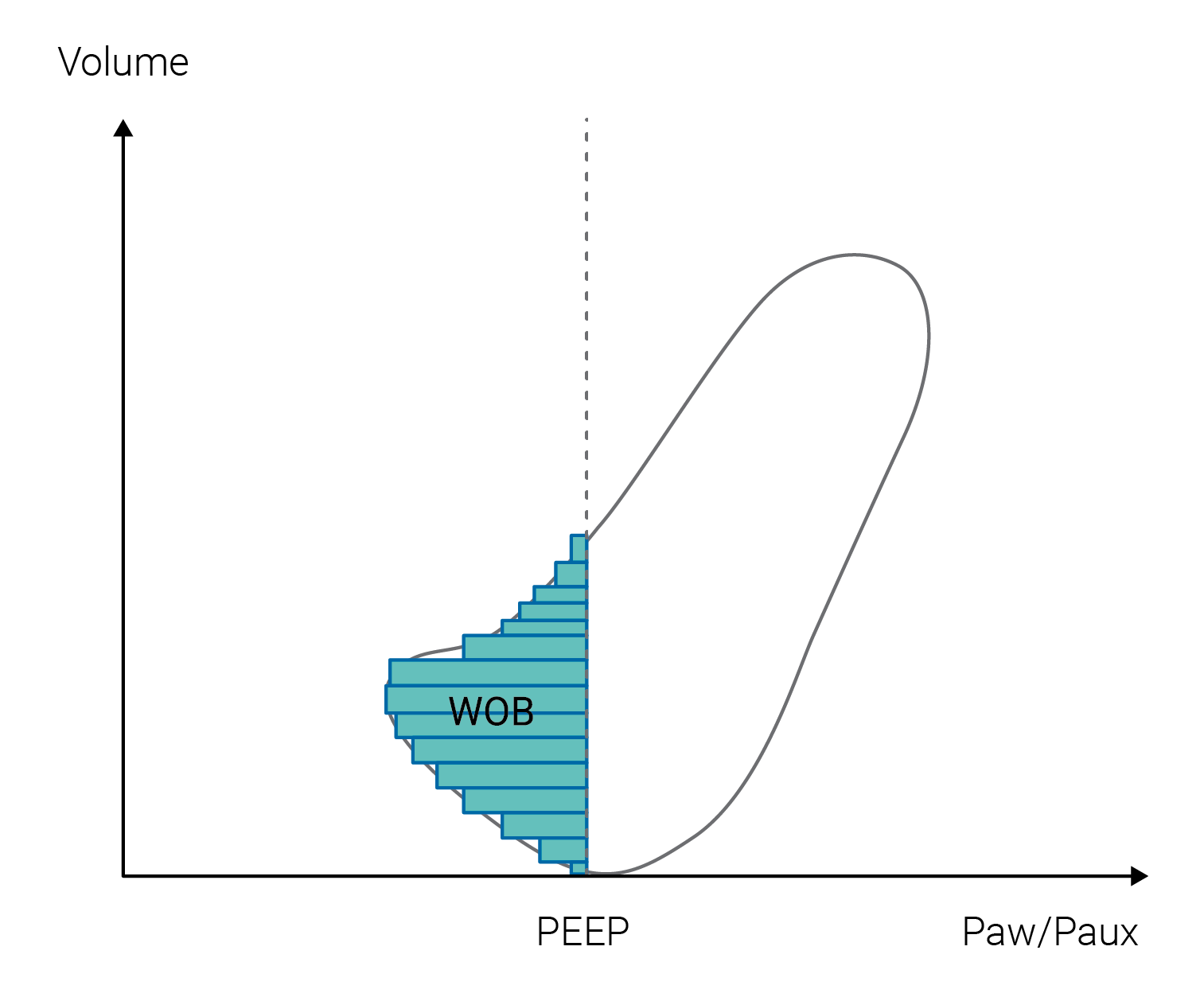
Work of breathing (WOB) represents the integral of the product of volume and pressure. It represents the energy associated with a given VT at a given pressure (spontaneous, mechanical, or both).
The airway pressure is the pressure of the whole respiratory system (lungs plus chest wall), the transpulmonary pressure is the pressure needed to distend the lung parenchyma, and the pleural pressure is the pressure needed to distend the chest wall.
In paralyzed patients with mechanical ventilation, plots of airway pressure versus VT indicate the total amount of work needed to inflate the respiratory system. This represents the work done by the ventilator on the whole respiratory system and the ETT, NOT the amount of work performed by the respiratory muscles.
Calculation of a patient’s WOB may be useful for understanding weaning failure, for helping in titrating ventilator support, and for evaluating the effects of different ventilation modes, the effects of therapeutic interventions, and the influence of ventilator performance (triggering, flow delivery, etc.).
For healthy people, the average total WOB ranges from 0.3 to 0.6 J/L. Patients with severe obstructive or restrictive lung disease “work” at levels two to three times this normal value at rest, with marked increases in work at higher minute ventilation (
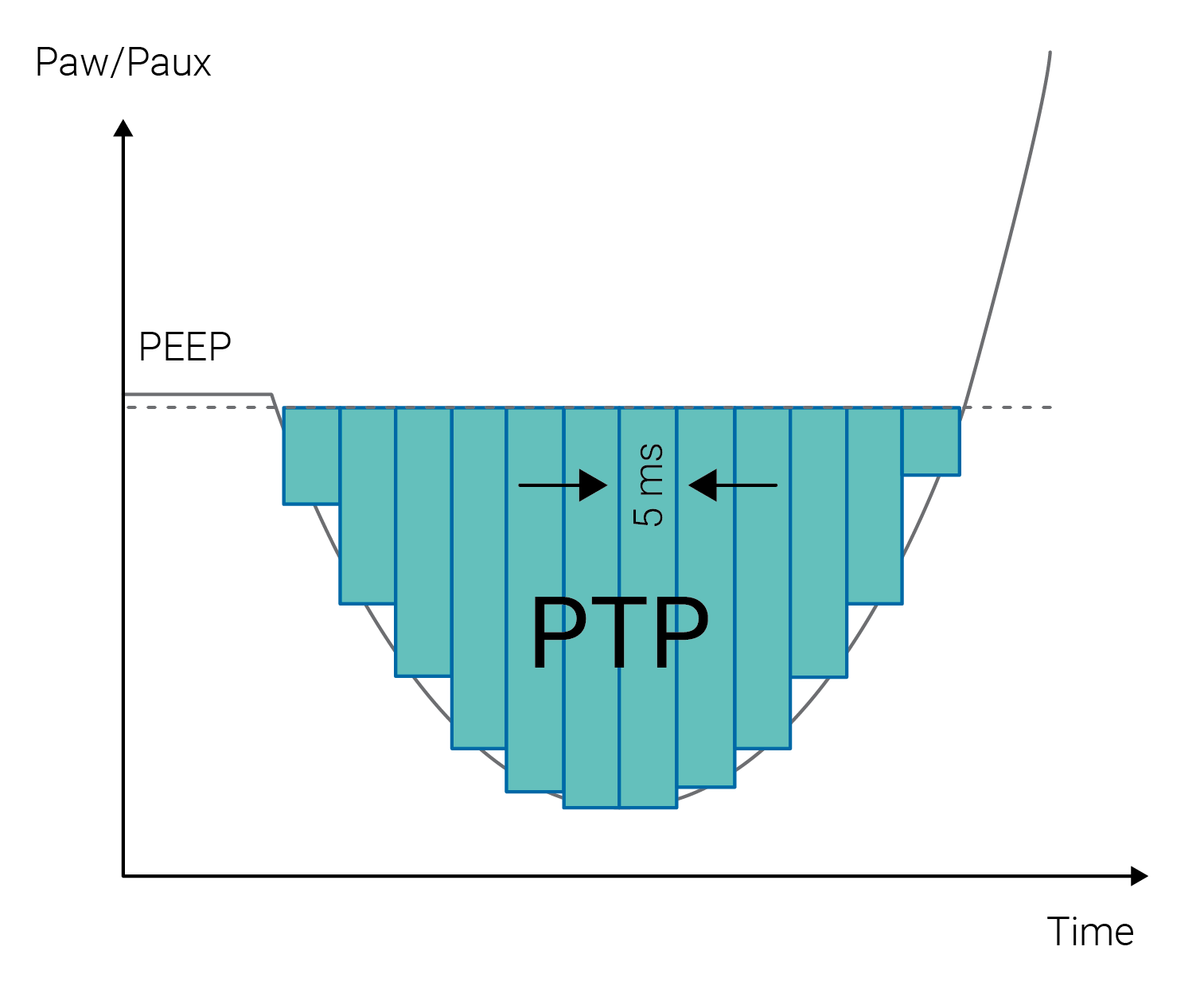
The pressure‑time product is the integral of the pressure performed by the respiratory muscles during inspiration. It is an alternative to WOB and has some theoretical and practical advantages over WOB calculations. The pressure‑time product (PTP) is the area encompassed by the esophageal or airway pressure time tracing during inspiration.
In principle, the HAMILTON‑G5/S1 ventilator measures the WOB for the patient only; this is valid for Paw and Paux (whichever is selected). WOB is airway pressure integrated over inspiratory volume until the pressure exceeds the PEEP/CPAP level. In the dynamic pressure/volume loop, WOB is the area to the left of PEEP/CPAP (as shown in Figure 1).
The PTP is the measured pressure drop required to trigger the breath multiplied by the time interval until the PEEP/CPAP level is reached at the beginning of inspiration. The PTP on Hamilton Medical ventilators is the area between PEEP and Paw or Paux/Pes (whichever is selected; Paux/Pes only for HAMILTON‑G5/S1 and HAMILTON‑C6, respectively), as long as Paw/Paux (Pes) is below PEEP as shown in Figure 2. Normal values for the pressure‑time product range between 60 and 150 cmH2O/second per minute.
Relevant ventilators: All
Relevant software: HAMILTON‑C1/T1/MR1 SW v2.2.4 and lower; HAMILTON‑C2 SW v 2.2.5 and lower; HAMILTON‑C3 SW v 2.0.5 and lower; HAMILTON‑G5/S1 SW v 2.81 and lower