Auteur: Munir Karjaghli, Kaouther Saihi
Date: 22.05.2023
In this article, we compare the various adaptive support ventilation modes available on the market.
Adaptive Support Ventilation® (ASV®) was the first commercially available adaptive ventilation mode to use an optimal targeting schema (
ASV is a closed‑loop ventilation mode that combines adaptive pressure‑controlled ventilation for passive patients, and adaptive pressure‑support ventilation for spontaneously breathing patients. This mode has the advantages of optimizing the patient's work and force of breathing, shortening the duration of mechanical ventilation supporting weaning and finally, reducing the workload of ICU staff while improving patient safety and comfort.
The ASV algorithm was originally based on the lowest work of breathing according to Otis' equation (
To reduce the tidal volume (and consequently the driving pressure), the ASV algorithm was modified in 2017 to incorporate Mead's equation for the lowest force of breathing (


This modification resulted in the new version 1.1, which is the default selection on all Hamilton Medical ventilators. The ASV 1.1 algorithm selects the optimal frequency at which the breathing power and force are lowest and thus delivers ventilation at a lower mechanical power (MP) (
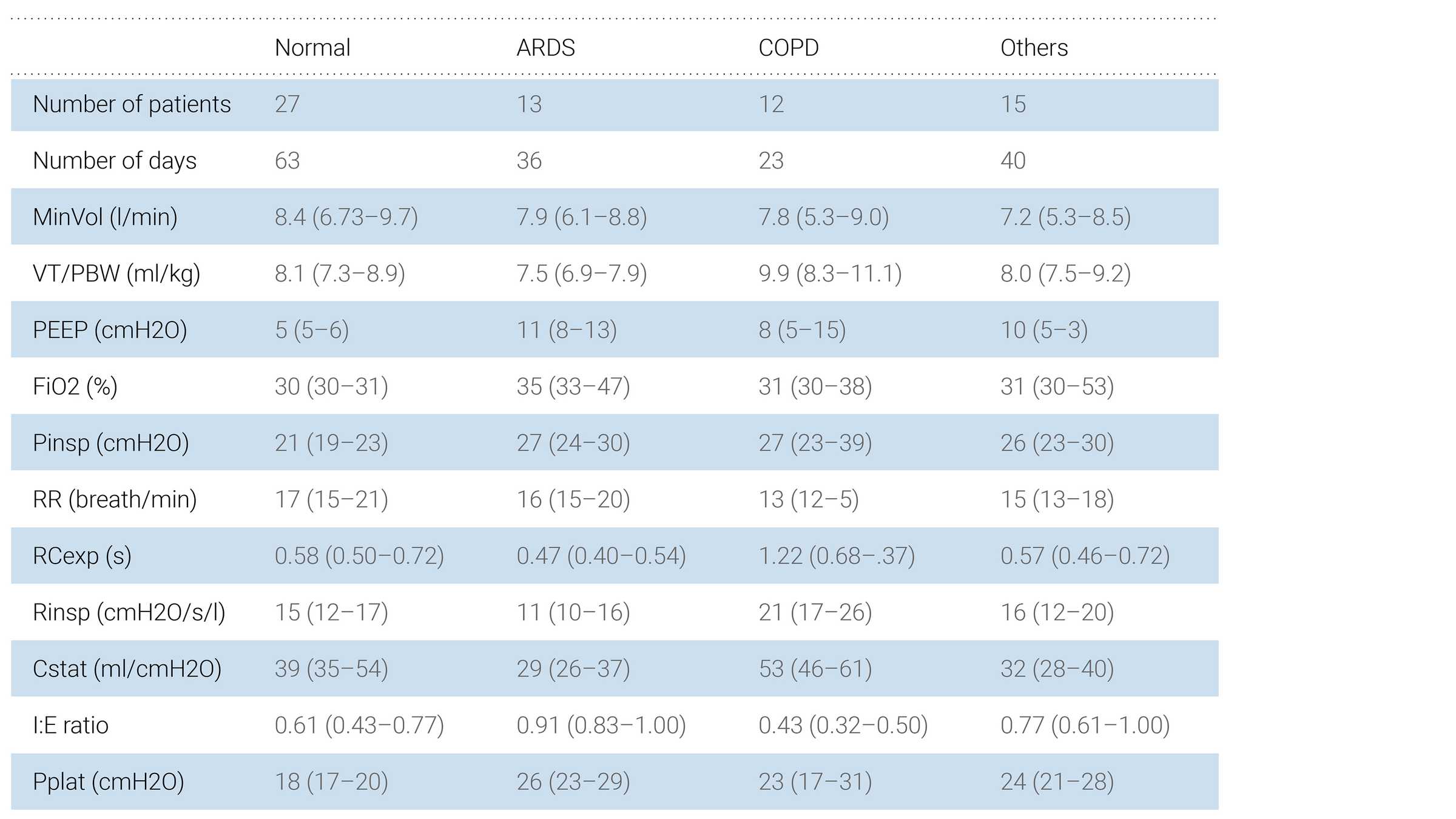
ASV 1.1 evaluates the patient's respiratory mechanics by measuring the expiratory time constant (RCexp) (
Recently, various other manufacturers have released adaptive ventilation modes similar to ASV 1.0, including “Adaptive Ventilation Mode” (IMT, Buchs, Switzerland), “Work of Breathing Optimized Ventilation” (Salvia Medical, Kronberg, Germany), and “Adaptive Minute Ventilation” (Mindray, Shenzhen, China). All these modes select a combination of RR and VT according to Otis’ equation and may therefore deliver a large VT, as observed in ASV by Dongelmans et al. (
The AVM algorithm was originally based on the lowest work of breathing according to Otis' equation as in the ASV mode. However, it was then modified in AVM2 to incorporate the concept of mean inspiratory power, whereby the optimal frequency is selected for the lowest inspiratory power. Inspiratory power is defined as the sum of the resistive and tidal power that is transmitted from the ventilator to the patient, assuming intrinsic PEEP is equal to zero.
AVM2 was announced in 2017 (
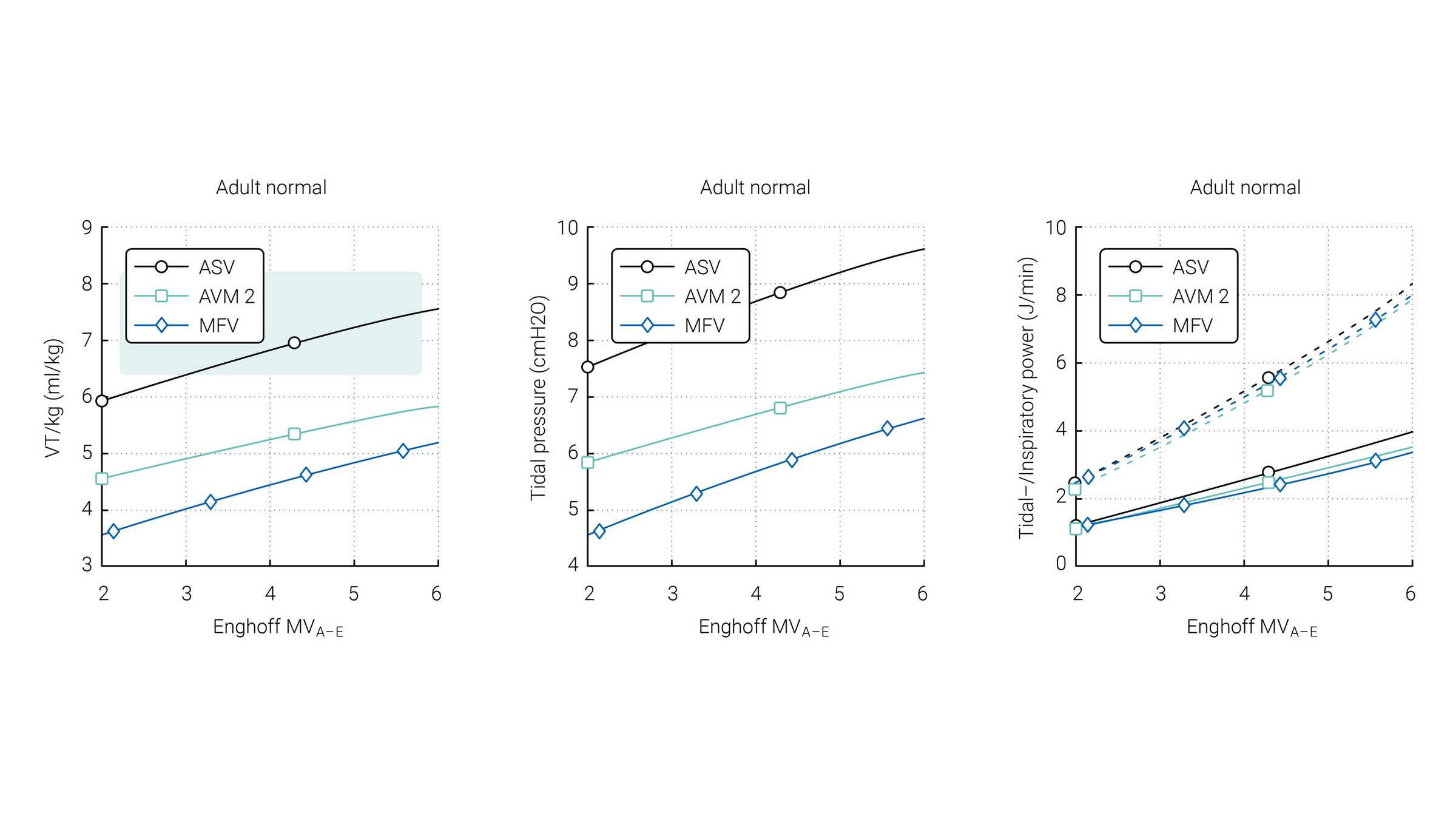
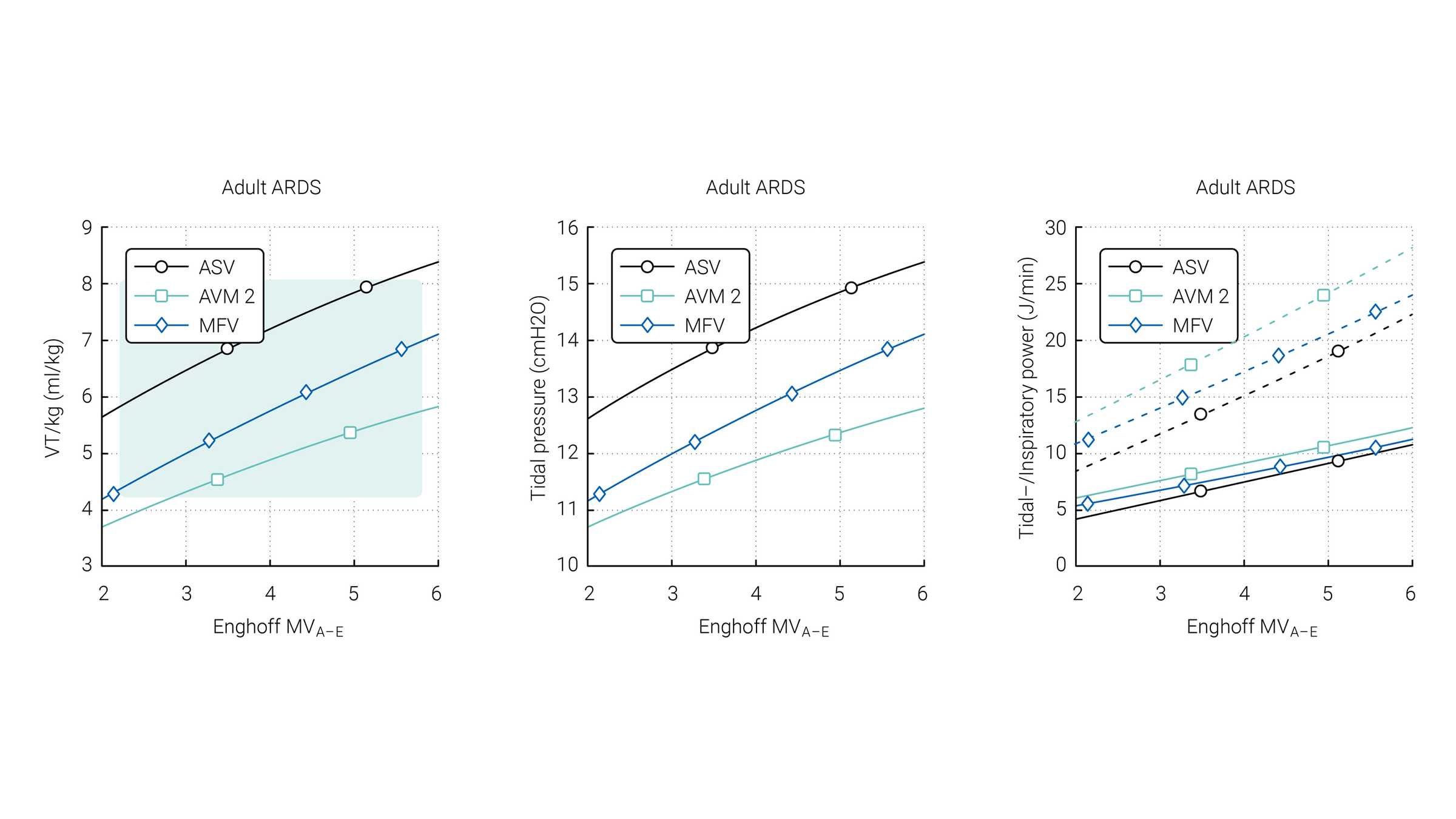
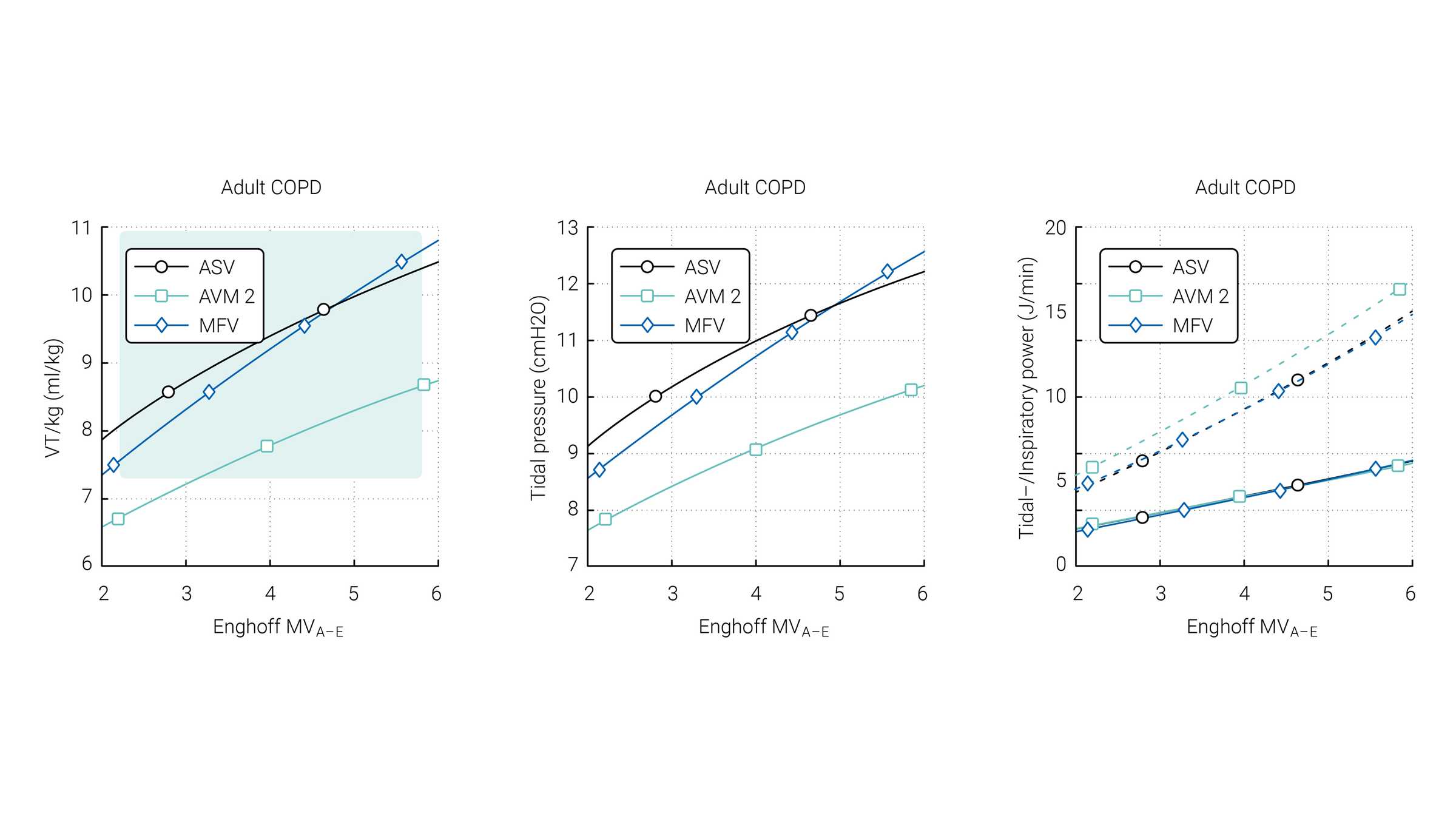
Van der Staay and Chatburn performed a comparison of three targeting schemes during selected simulation scenarios with ASV 1.0, AVM2, and MFV (
The green area highlights the range which is normally used for these patients according to Arnal et al. (



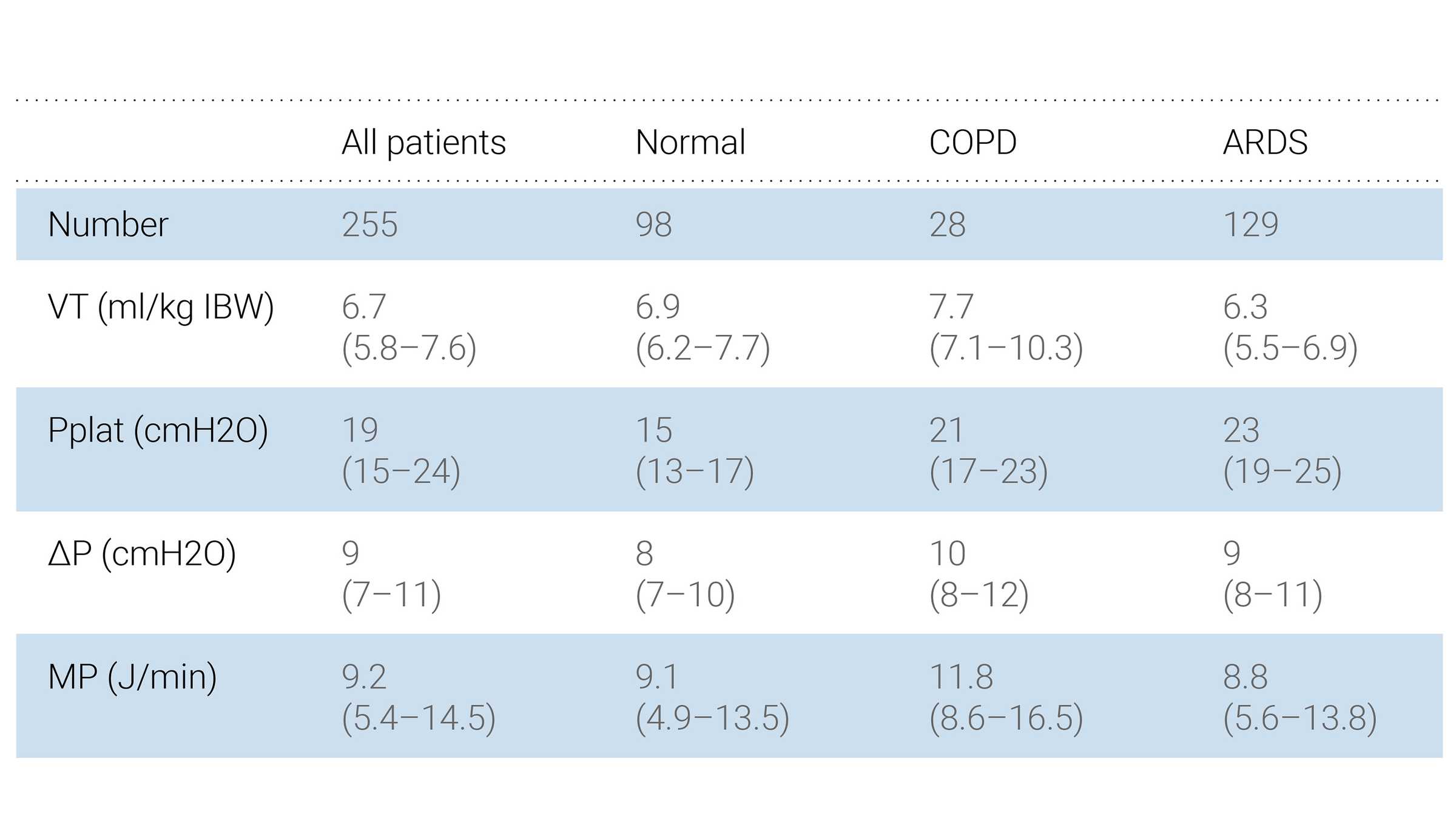
Several studies have been conducted to investigate the benefits of ASV 1.1 over conventional modes. These studies show that ASV 1.1 can select individualized VT‑RR combinations, and reduce the metabolic load and mechanical power delivered to the patient when compared to conventional ventilation modes (