

Autore: Caroline Brown, Giorgio Iotti
Data: 08.07.2022
L'asincronia tra paziente e ventilatore è un'eventualità comune nei pazienti ventilati meccanicamente (1, 2).
La mancata corrispondenza tra i tempi inspiratori ed espiratori di paziente e ventilatore può presentarsi sotto diverse forme, per esempio come ciclaggio ritardato, trigger automatico, doppio trigger o sforzo inefficace, ed è stato evidenziato che questa situazione ha un impatto sugli esiti dei pazienti (
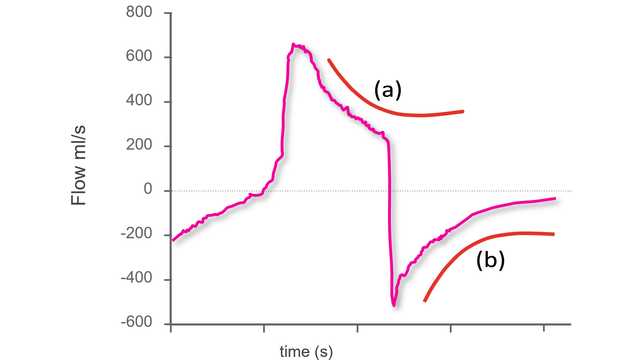
L'ipotesi di analizzare le curve di flusso e pressione delle vie aeree per rilevare gli sforzi espiratori e i relativi tempi è stata avanzata quasi trent'anni fa (
Un elemento chiave di questa sperimentazione è stato l'utilizzo di un metodo sistematico per l'analisi delle curve di flusso e pressione delle vie aeree, costituito da cinque principi generali e una serie di regole specifiche definite in anticipo (che chiameremo "il metodo delle curve"). Tutti i pazienti erano ventilati in modalità a supporto di pressione con un catetere esofageo posizionato. Il metodo è stato applicato alle curve del flusso e della pressione delle vie aeree ottenute tramite un sensore prossimale; la pressione esofagea (Pes) è stata utilizzata come punto di riferimento. Per ogni paziente, tre ricercatori presi da un gruppo di quattro (tre medici senior e uno specializzando) hanno analizzato solo le curve di flusso e pressione, mentre il quarto ricercatore ha analizzato sia le curve di flusso e pressione sia la curva della Pes. I respiri sono stati classificati come normalmente assistiti, a trigger automatico, a doppio trigger o sforzi inefficaci. Nel caso dei respiri normalmente assistiti, sono state valutate anche le asincronie lievi (ritardo del trigger, ciclaggio prematuro e ciclaggio ritardato).
L'endpoint primario era la percentuale di sforzi spontanei rilevati utilizzando il metodo delle curve. Tra gli endpoint secondari sono stati inclusi l'accordo tra il metodo delle curve e il metodo di riferimento per quanto riguarda la rilevazione di sincronie maggiori e minori, oltre all'accordo reciproco delle valutazioni eseguite con il metodo delle curve da diversi valutatori.
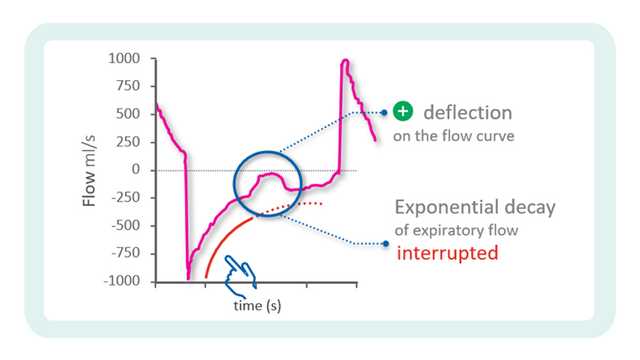
Sono stati registrati in totale 4.426 respiri. Utilizzando le misure di riferimento derivate dalla Pes, il 77,8% dei respiri è stato identificato come respiro correttamente rilevato dal ventilatore, il 22,1% come sforzo inefficace e lo 0,1% come respiro a trigger automatico. Con il metodo delle curve è stato possibile rilevare il 99,5% degli sforzi spontanei e tutti i respiri a trigger automatico tranne uno. L'accordo tra il metodo di riferimento e il metodo delle curve è stato molto elevato anche per la classificazione dei respiri come assistiti, a trigger automatico, a doppio trigger o sforzi inefficaci. L'indice di asincronia, calcolato come la somma dei respiri a trigger automatico, a doppio trigger e inefficaci divisa per il numero totale di respiri, è risultato pari a 5,9% e il valore ottenuto è stato il medesimo con il metodo delle curve e con quello della pressione esofagea. Il tempo di asincronia totale, calcolato come il tempo durante il quale paziente e ventilatore non erano sincronizzati diviso per il tempo di registrazione complessivo, era del 22,4%, con una componente del 92,1% dovuta alle asincronie lievi. Anche l'accordo tra i diversi operatori nella classificazione dei respiri è stato molto elevato.
In oltre il 90% dei casi, il metodo delle curve ha consentito ai ricercatori di identificare l'inizio e la fine degli sforzi respiratori con una precisione sufficiente a classificare correttamente anche le asincronie lievi (trigger ritardato, ciclaggio prematuro e ciclaggio ritardato).
Questo studio ha ottenuto alcuni importanti risultati Gli sperimentatori hanno evidenziato che il metodo delle curve consente ai medici di rilevare una percentuale molto alta degli sforzi respiratori spontanei e di valutare con precisione i tempi dell'attività del paziente. Anche nel caso di asincronie lievi, il metodo delle curve risulta altamente affidabile e riproducibile. L'importanza di questo risultato è sottolineata da un ulteriore dato rilevato dallo studio: la maggior parte del tempo di asincronia in modalità PSV era dovuto ad asincronie minori.
Non solo questi risultati dimostrano la riproducibilità del metodo delle curve (con un'elevato accordo inter‑operatore) ma evidenziano anche che una formazione nell'analisi delle curve secondo un metodo predefinito e sistematico gioca un ruolo fondamentale. Le evidenze hanno dimostrato che l'esperienza clinica nel trattamento dei pazienti ventilati meccanicamente non equivale necessariamente alla capacità di riconoscere le asincronie, che è complessivamente poco comune nei medici di terapia intensiva (
Gli autori concludono che le curve di flusso d'aria e pressione delle vie aeree misurate a livello prossimale contengono informazioni sufficienti per valutare in modo accurato l'attività del paziente e l'interazione paziente‑ventilatore, ipotizzando che si adotti un metodo di analisi sistematico adeguato, come il "metodo delle curve".
La tecnologia IntelliSync®+ integrata nei ventilatori Hamilton Medical (
Citazioni complete a fondo pagina: (

La nostra scheda di riferimento sulle asincronie fornisce una panoramica sui tipi più comuni di asincronie, sulle loro cause e su come individuarle.
The first step to identifying asynchronies using standard ventilator waveforms is knowing what a synchronous breath looks like during pressure‑support ventilation.
In the previous issue, our Bedside tip covered the starting point for identifying asynchronies using ventilator waveforms.
