Автор: Жан‑Пьер Ревелли (Jean‑Pierre Revelly), Джорджио Иотти (Giorgio Iotti)
Дата: 03.04.2023
В этой статье более подробно рассматриваются различные компоненты механической мощности, их значение в клинических условиях и использование в качестве мониторируемых параметров.
В этой статье рассматривается только механическая мощность (MP) во время фазы вдоха при искусственной вентиляции при условии отсутствия дыхательного усилия пациента.
В физике:
При механической вентиляции мощность, передаваемая от аппарата ИВЛ к дыхательной системе во время вдоха, представляет собой комплексную переменную, объединяющую элементы, которые могут вызывать вентилятор‑индуцированное повреждение легких (ВИПЛ) (
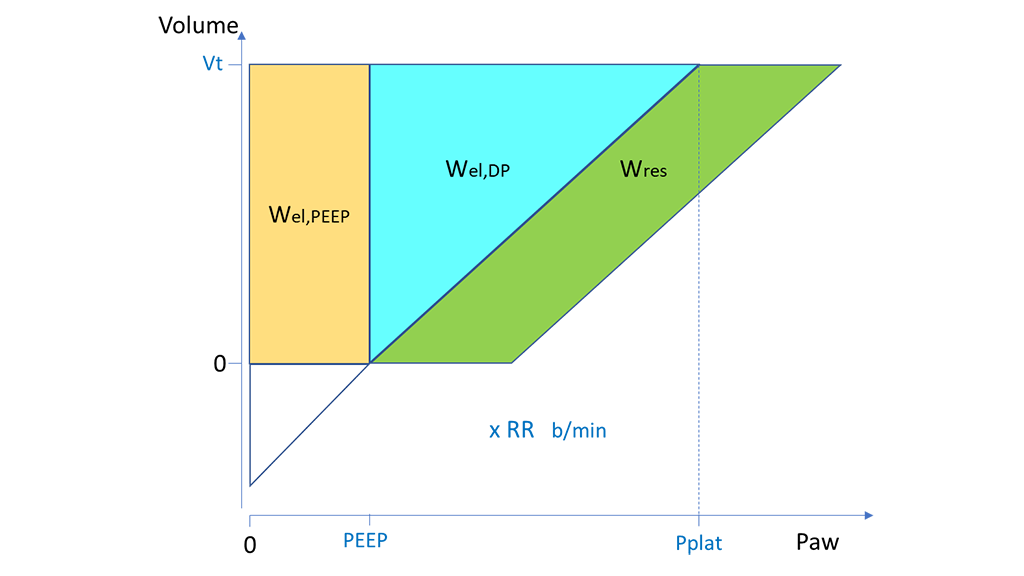
Во время управляемой принудительной вентиляции (CMV) с постоянным потоком механическую мощность можно описать как работу за один вдох (W), умноженную на частоту дыхания (RR) (рис. 1). (
Где:

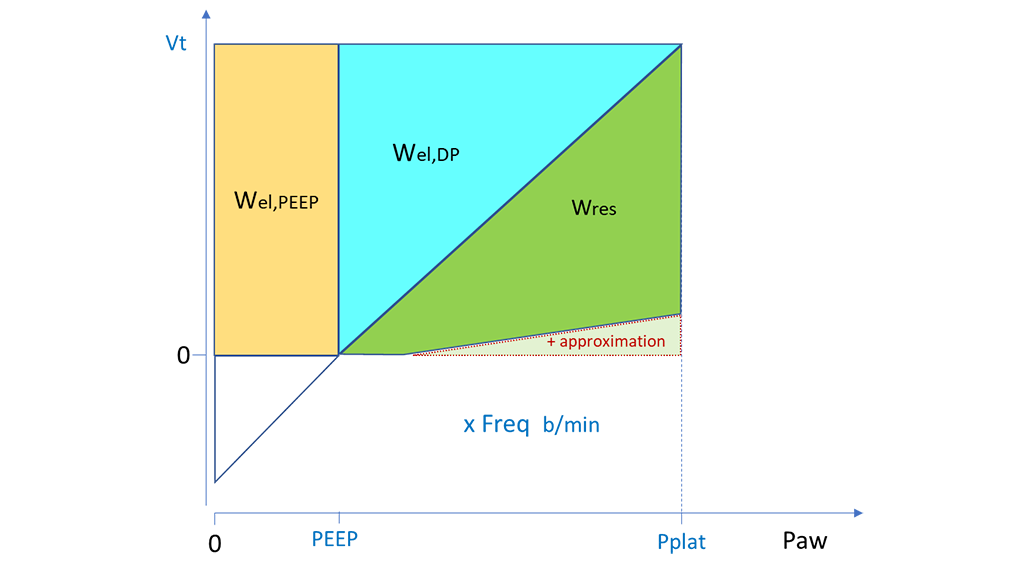
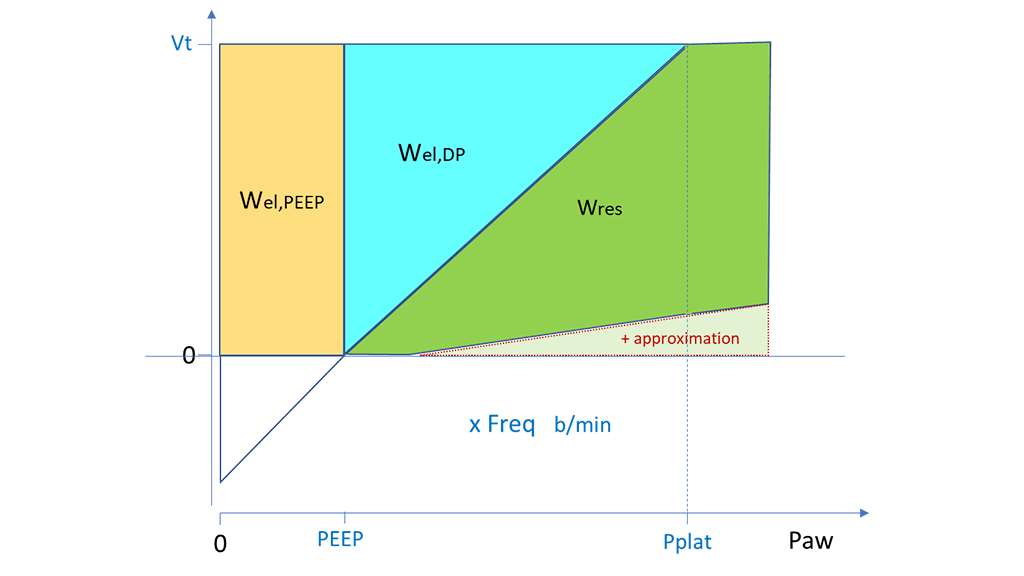
Аналогичный подход можно применять во время вентиляции с управлением по давлению (PCV) для расчета значений «Wel,PEEP» и «Wel,DP» на основе показателей «Vt», «PEEP» и «DP». Значение «Wres» можно рассчитать приблизительно. Для этого следует вычислить площадь прямоугольника (с «Pпик» минус «PEEP» в качестве основания и «Vt» в качестве высоты), а затем вычесть треугольник, соответствующий «Wel,DP». Этот расчет значения «Wres» можно применять таким же образом, когда значение «Pпик» равно значению «Pплато» (рис. 2) или превышает его (рис. 3), т. е. когда поток в конце вдоха равен нулю или, соответственно, все еще имеет положительное значение. В обоих случаях приблизительный расчет приводит к небольшому завышению значения «Wres» и, следовательно, истинного значения полной работы аппарата ИВЛ (


Значительное количество исследователей рассчитывали механическую мощность по данным исследований вентиляции у находящихся в отделениях интенсивной терапии пациентов с (
Ниже приведены данные из этих аналитических материалов.
В целом эти ретроспективные исследования дают основание считать, что чрезмерной механической мощности предпочтительно избегать, если предположить, что худший клинический исход был частично связан с вентилятор‑индуцированным повреждением легких.
Чтобы правильно понять методы расчета механической мощности, использованные в опубликованных исследованиях, их необходимо тщательно изучить. В зависимости от имеющихся данных авторы могли учесть или исключить некоторые компоненты механической мощности. Кроме того, наиболее подходящая процедура для сравнения разных пациентов все еще является предметом обсуждения. Предлагается стандартизировать параметры пациента (прогнозируемый вес), податливость или объем легких в конце выдоха.
В принципе, в настоящее время еще не существует ни стандартизированного подхода к расчету механической мощности, ни ее общепризнанного безопасного расчетного значения.
Отдельные изменения параметров аппарата ИВЛ оказывают сложное влияние на другие переменные механики вентиляции. Концепция механической мощности основана на неявном допущении того, что все переменные вентиляции имеют линейное соотношение и одинаковую связь с ВИПЛ. Однако это, очевидно, ошибочное предположение, поскольку, например, параметр «PEEP» имеет криволинейную (J‑образную) связь с ВИПЛ (
Несмотря на то, что многие вопросы остаются открытыми, мониторинг общей механической мощности и ее компонентов может оказаться полезным для оценки динамики отдельных пациентов или их реакции на изменения параметров вентиляции. Механическая мощность может стать новым критерием (наряду с несколькими другими) в клинической оценке и принятии решений. Более того, мониторинг механической мощности в значительной степени поможет в сборе высококачественных данных для всех проспективных исследований взаимосвязи между механической мощностью и ВИПЛ.
Различные исследователи делали попытки выявить наиболее вредные компоненты вентиляции. В ретроспективном исследовании были собраны данные об ИВЛ у 4500 пациентов с ОРДС, включенных в контролируемые исследования. В процессе исследования оценивалась взаимосвязь механической мощности, показателей «Vt», «RR» и «DP» со смертностью в течение 28 дней, для чего использовались многопараметрические модели (
Неудивительно, что авторы выявили связь общей механической мощности со смертностью. При оценке различных компонентов механической мощности статистически значимым был только гибкий динамический компонент («MPel,DP», т. е. механическая мощность, которая зависит от показателя «Wel,DP»), а компоненты, зависящие от показателя «PEEP» или сопротивления, ‑ не были. Значение «MPel,DP» особенно легко рассчитать у постели больного в обоих режимах: CMV и PCV.
Более того, авторы обнаружили аналогичный прогноз смертности, просто объединив показатели «DP» и «RR» в следующем индексе:
Авторы пришли к выводу, что «хотя механическая мощность была связана со смертностью у пациентов с ОРДС, показатели «∆P» и «RR» были столь же информативны, их было легче оценить у постели больного. Влияние стратегии вентиляции, основанной на этих переменных, на исход заболевания необходимо проверить в рандомизированных контролируемых исследованиях» (