Author: Kathrin Seeger, ICU nurse, Hamilton Medical Clinical Application Specialist
Date of first publication: 12.06.2024
Everything healthcare professionals need to know to get started with high flow nasal cannula therapy: the flow rate, FiO2 settings, when to use HFNC, selecting the interface, and much more.
There is a range of terminology used for high flow nasal cannula (HFNC) therapy: HFNC supportive therapy, high flow therapy (HFT), nasal high flow (NHF), high flow (HF), high flow nasal cannula oxygen therapy, heated humidified high flow therapy (HHHF), high flow oxygen (HFO) therapy, and high flow oxygen therapy (HFOT). Hamilton Medical uses the term high flow nasal cannula (HFNC) therapy.
Good to know: The term HFNC refers to the therapy itself irrespective of the interface used (nasal cannula or tracheostomy connector).

High flow nasal cannula therapy is a type of respiratory support that delivers heated and humidified gas with a controlled concentration of oxygen to your patients. This therapy has become increasingly popular for hypoxemic respiratory failure.
HFNC is used during early noninvasive management of acute respiratory failure, and has proven to be safe and effective as a noninvasive ventilation method. HFNC has been shown to be potentially useful and efficient in other applications such as major postoperative care, immunocompromised patients, for preoxygenation, or during bronchoscopy (
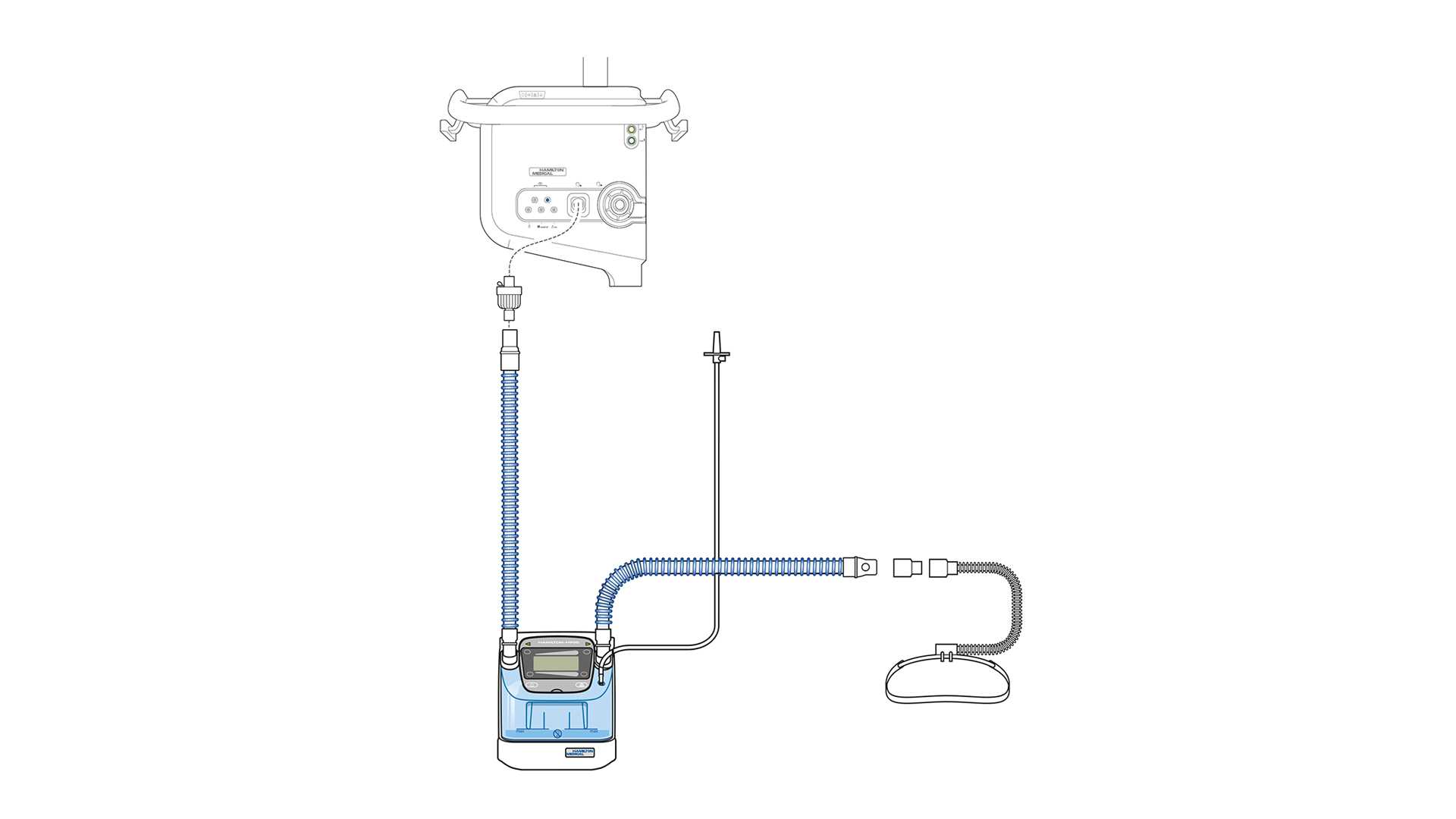
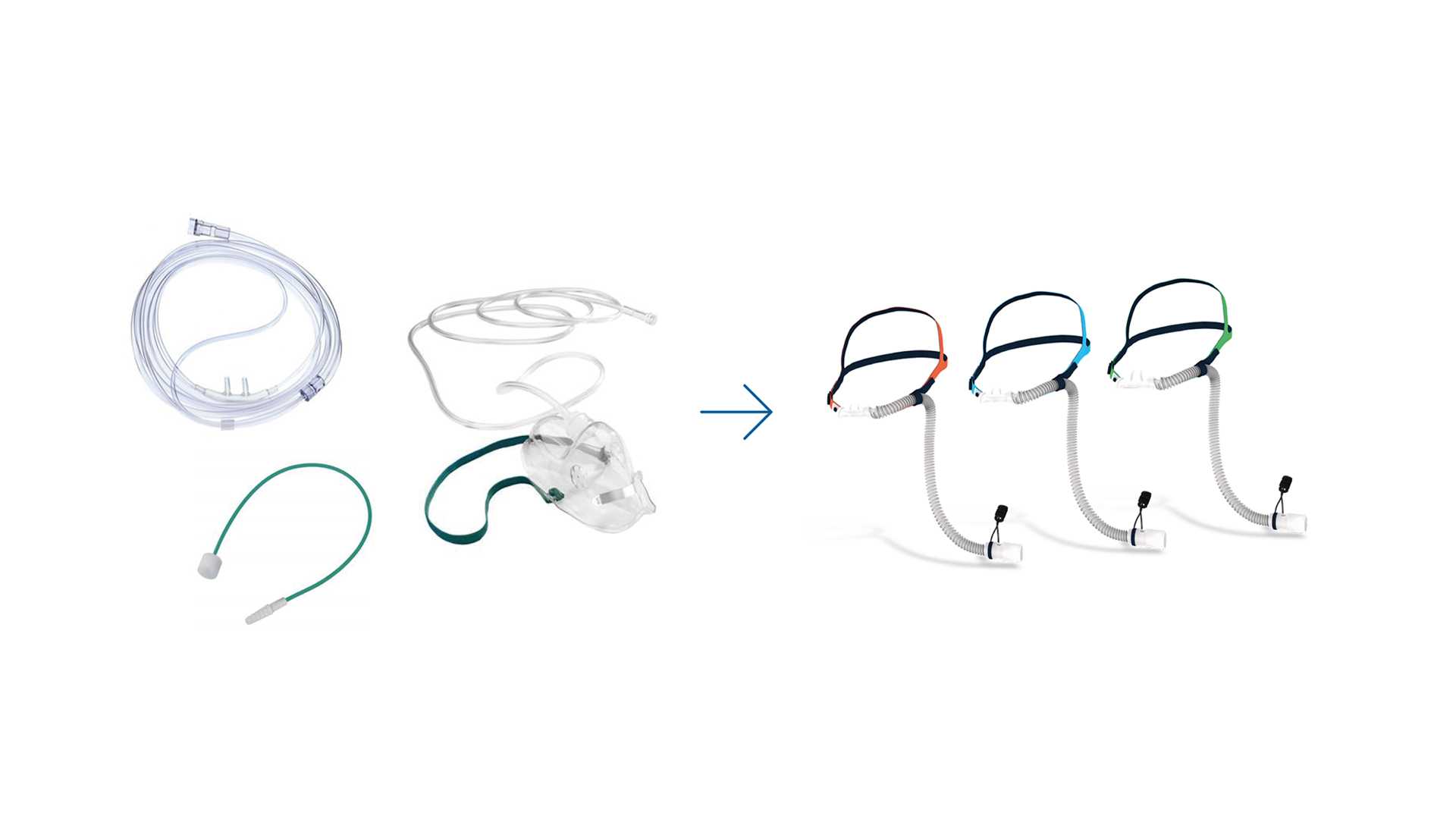
The system used to deliver HFNC requires the following components: a gas blender and flow meter, an active humidifier, a heated inspiratory circuit, and a nasal cannula or a tracheostomy connector as an interface. When we talk about high flow nasal cannula, we need to keep in mind the four elements that describe this therapy: flow, oxygen, heat, and humidity.
If we take a closer look at the meaning of each element, the advantages of using HFNC are clear:
Good to know: Did you know that the inspiratory demands of adult patients with acute respiratory failure can range from 30 l/min to more than 120 l/min?



We can divide the benefits of HFNC into clinical and physiologic as follows.
Clinical benefits:
Physiologic benefits:

Before we dive into the working principles of high flow nasal cannula, we need to address the limitations that are typical of low flow oxygen delivery systems. This will help you better understand the beneficial effects of HFNC for your patients.
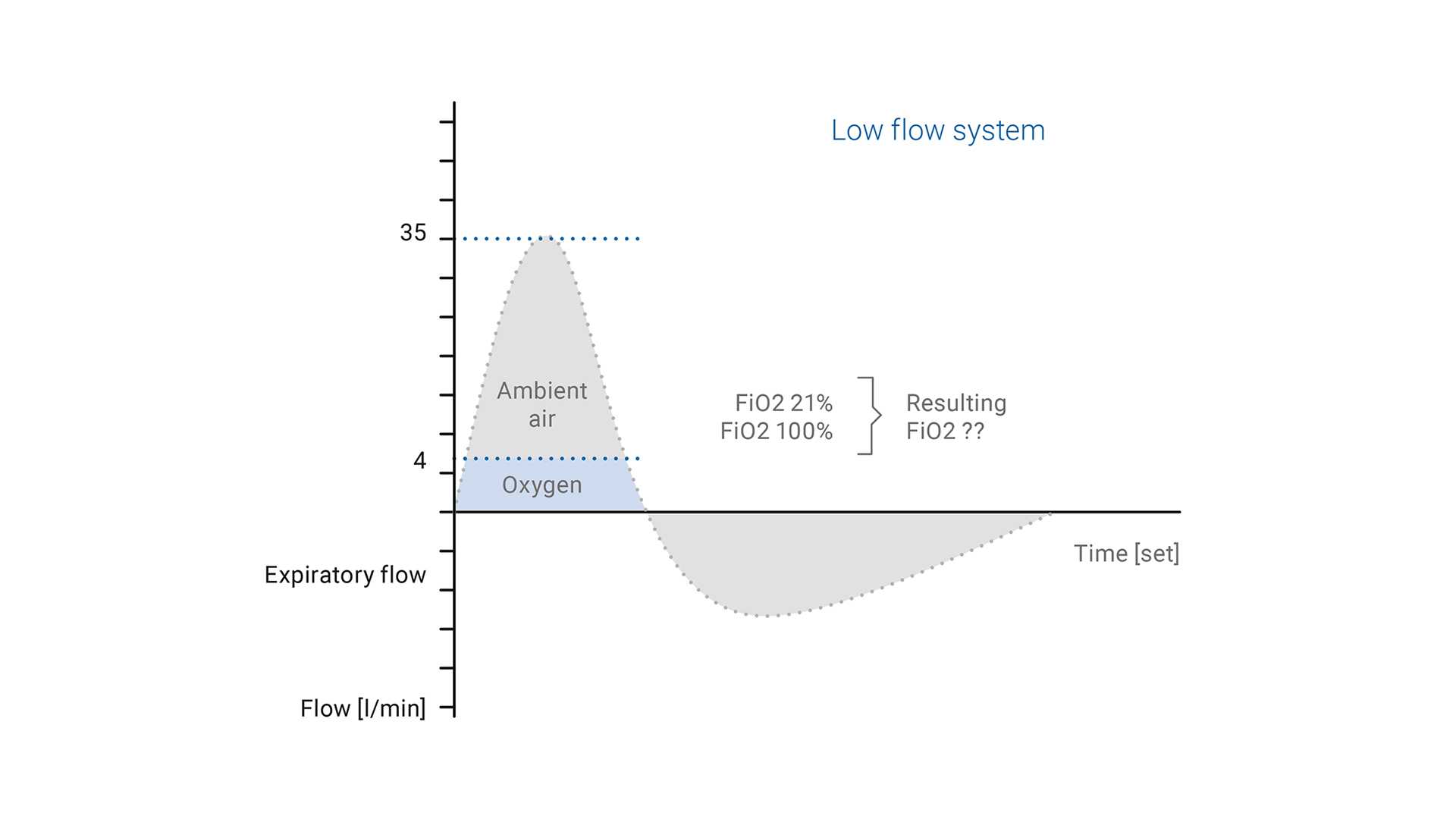
With conventional oxygen delivery devices, the peak inspiratory flow rate in acute respiratory failure patients exceeds the delivered flow of oxygen. Typical low flow systems provide supplemental O2 directly to the airway at a flow of 8 l/min or less. This O2 provided by a low flow device is always diluted with ambient air (with 21% FiO2); the result is a low and variable FiO2.
This variable FiO2 may be associated with one or more of the following: the interface used to deliver oxygen, the respiratory rate, the peak inspiratory flow and how the patient breathes (through the mouth or nose).
Good to know: The use of humidification is recommended when oxygen is supplied through a nasal cannula at flow rates of more than 4 l/min.

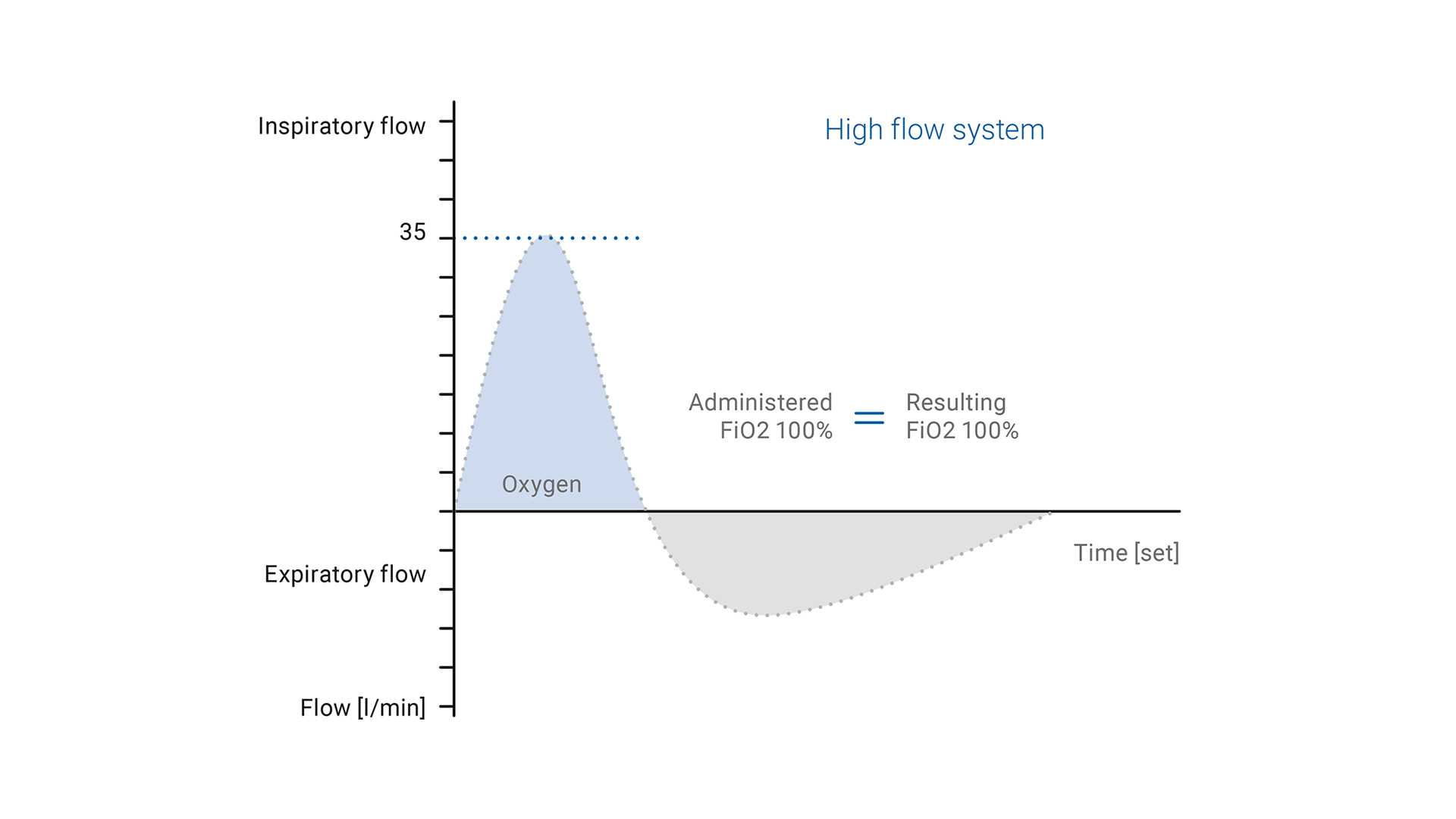
In contrast to low flow oxygen therapy, the gas flow rate and FiO2 in HFNC can be adjusted independently of one another, depending on the patient‘s inspiratory demands.
With high flow nasal cannula systems, the FiO2 is delivered more accurately and can be set from 21% to 100%.
As mentioned already, the higher flow rates are able to meet or even exceed the patient‘s peak inspiratory flow rate.
The blend of air and oxygen delivered to the patient is fully heated and humidified by the humidification chamber and the single limb heated breathing circuit. This breathing circuit contains heater wires within the tubing wall that minimize condensation.
The therapy is delivered directly into the patient‘s nostrils through a nasal cannula.
During normal inspiration, the PIF demand is 30 to 40 l/min. With high flow nasal cannula therapy, the administered FiO2 would equal the inhaled FiO2, while in the case of a low flow system, the inhaled FiO2 would be less than the administered FiO2 because it is diluted with ambient air (
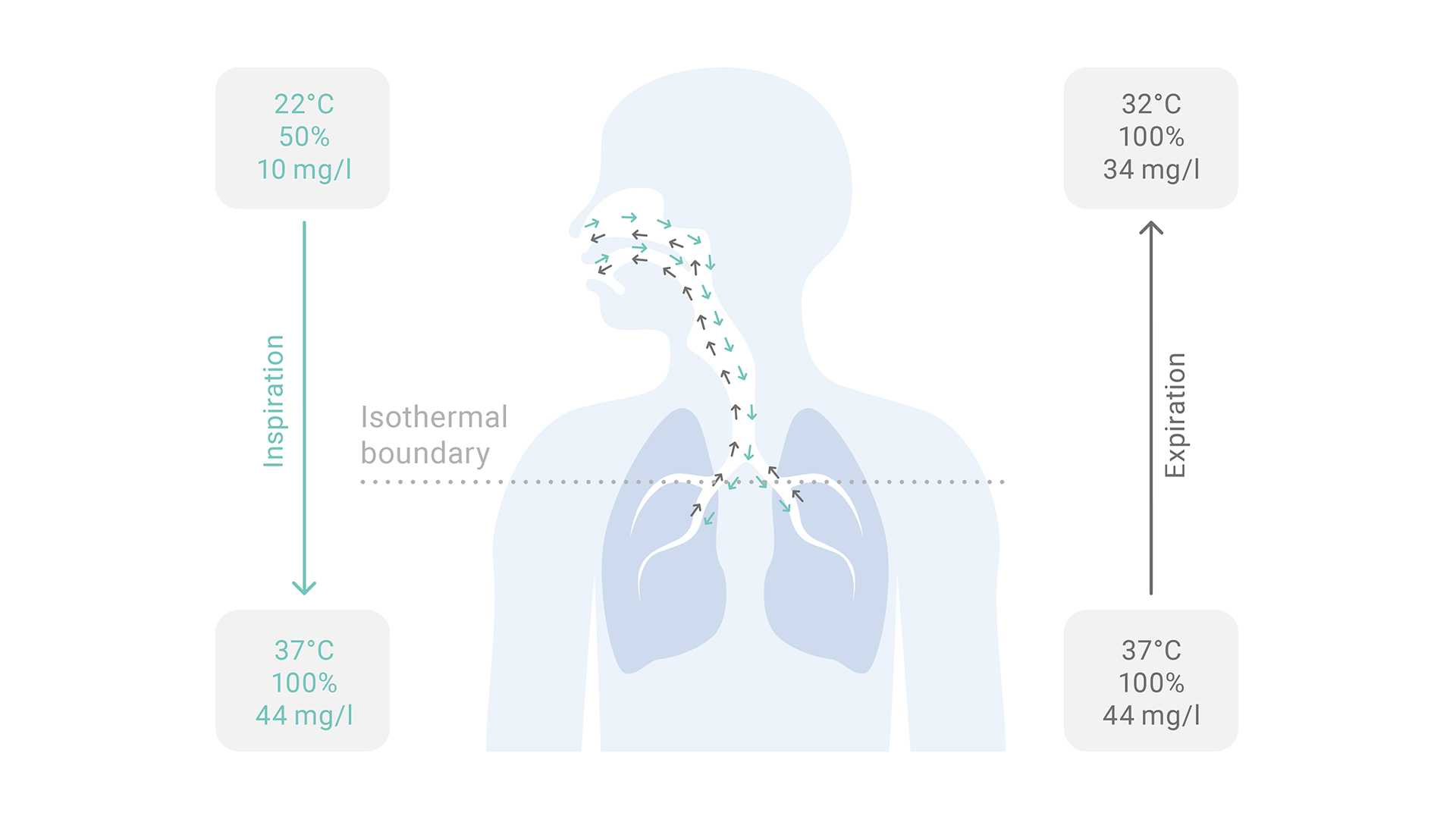
For higher flows, adequate humidification is fundamental because it improves the tolerance and compliance of the treatment. HFNC systems require an active heated humidifier to achieve optimal body temperature (37°C in adults and 34°C to 37°C in pediatric patients) with a humidity output of higher than 33 mg H2O/l and close to 100% of relative humidity.
The conditions provided by HFNC promote:



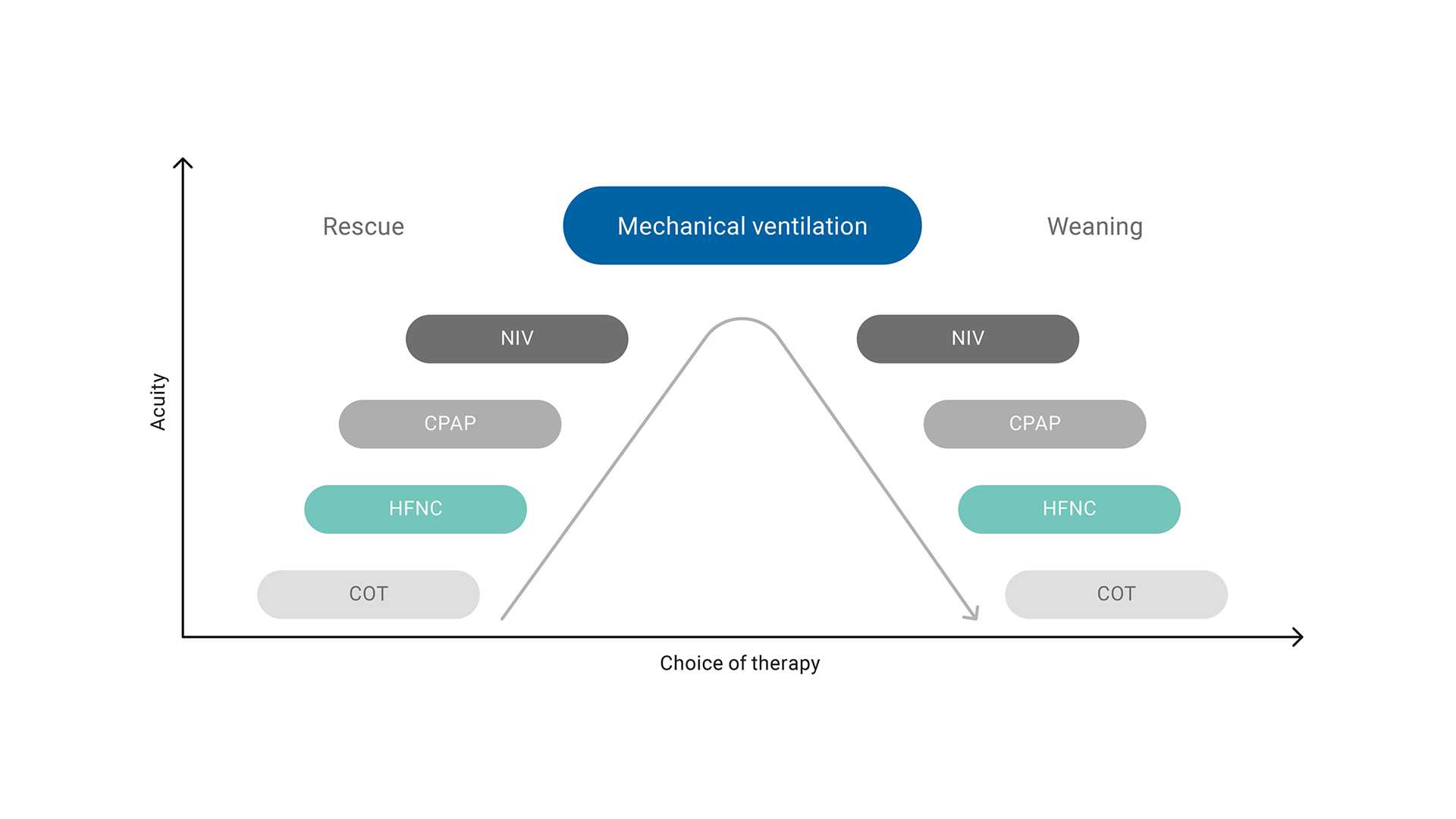
HFNC is considered the first‑line therapy for patients with acute hypoxemic respiratory failure and can be part of a treatment strategy, whether during escalation or weaning.

(
| Clinical indication | Recommendation | Comments |
| Hypoxemic respiratory failure | Strong recommendation |
|
| Post‑extubation | Conditional recommendation |
|
| Post‑operative HFNC in high risk and/or obese patients following cardiac or thoracic surgery | Conditional recommendation |
|
| Peri‑intubation period | No recommendation |
|

Negative end‑expiratory transpulmonary pressure can cause ventilator‑induced lung injury due to atelectrauma. Studies (
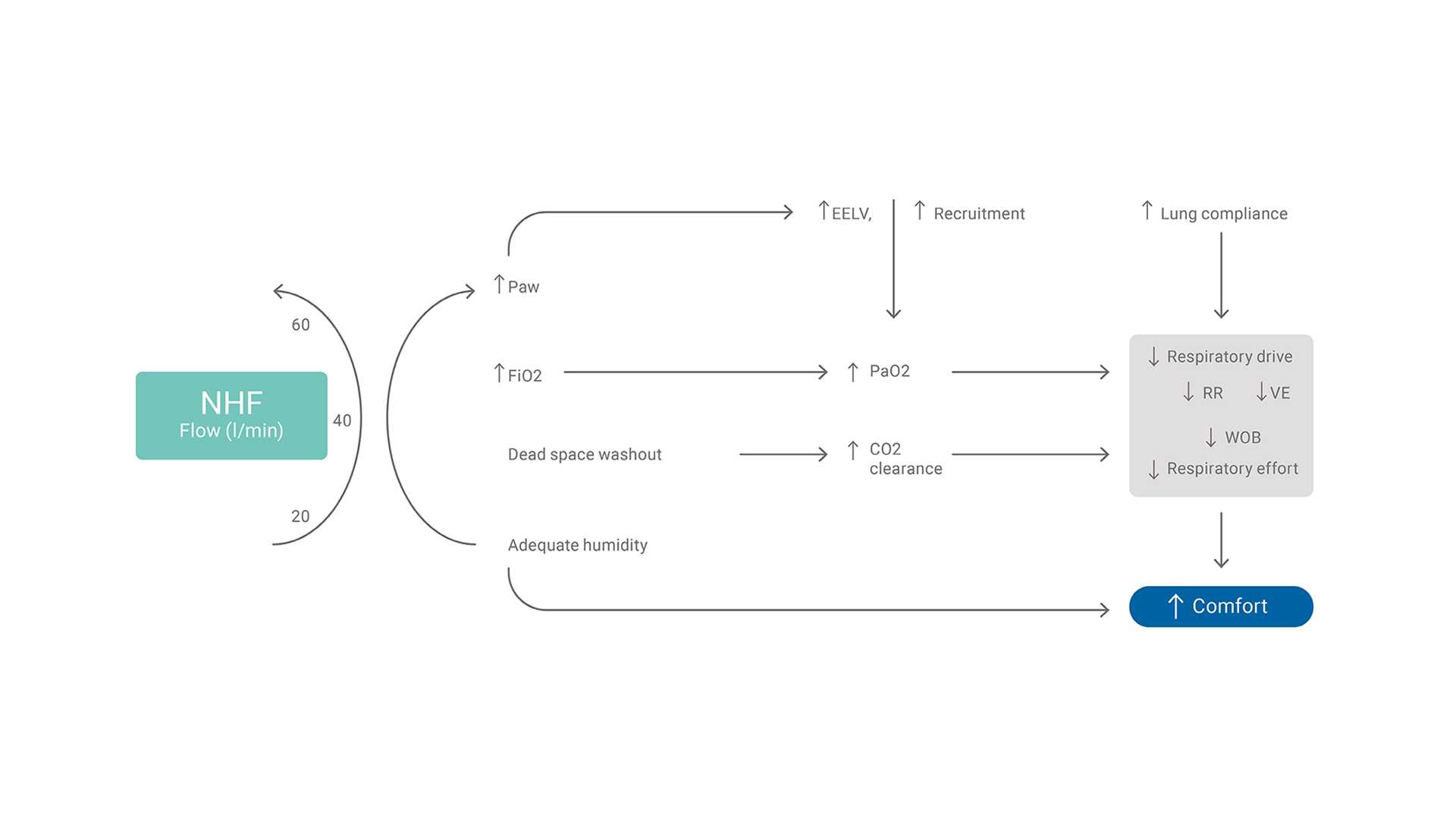
Amongst the main physiologic effects of HFNC are an increase in airway pressure and end‑expiratory lung volume (EELV), and an improvement in oxygenation. These are more evident with higher flows of around 60 to 70 l/min. However, the beneficial effects on parameters such as dead‑space washout, work of breathing, and respiratory rate may be achieved with intermediate flows (20 to 45 l/min)6.
Good to know: The physiologic effects of HFNC can be summarized as improved oxygenation, reduced work of breathing, improved lung protection and better comfort for the patient.


Discover the all‑in‑one solution for high flow oxygen therapy, providing caregivers with the tools and flexibility needed to tailor treatment to each patient’s unique needs.

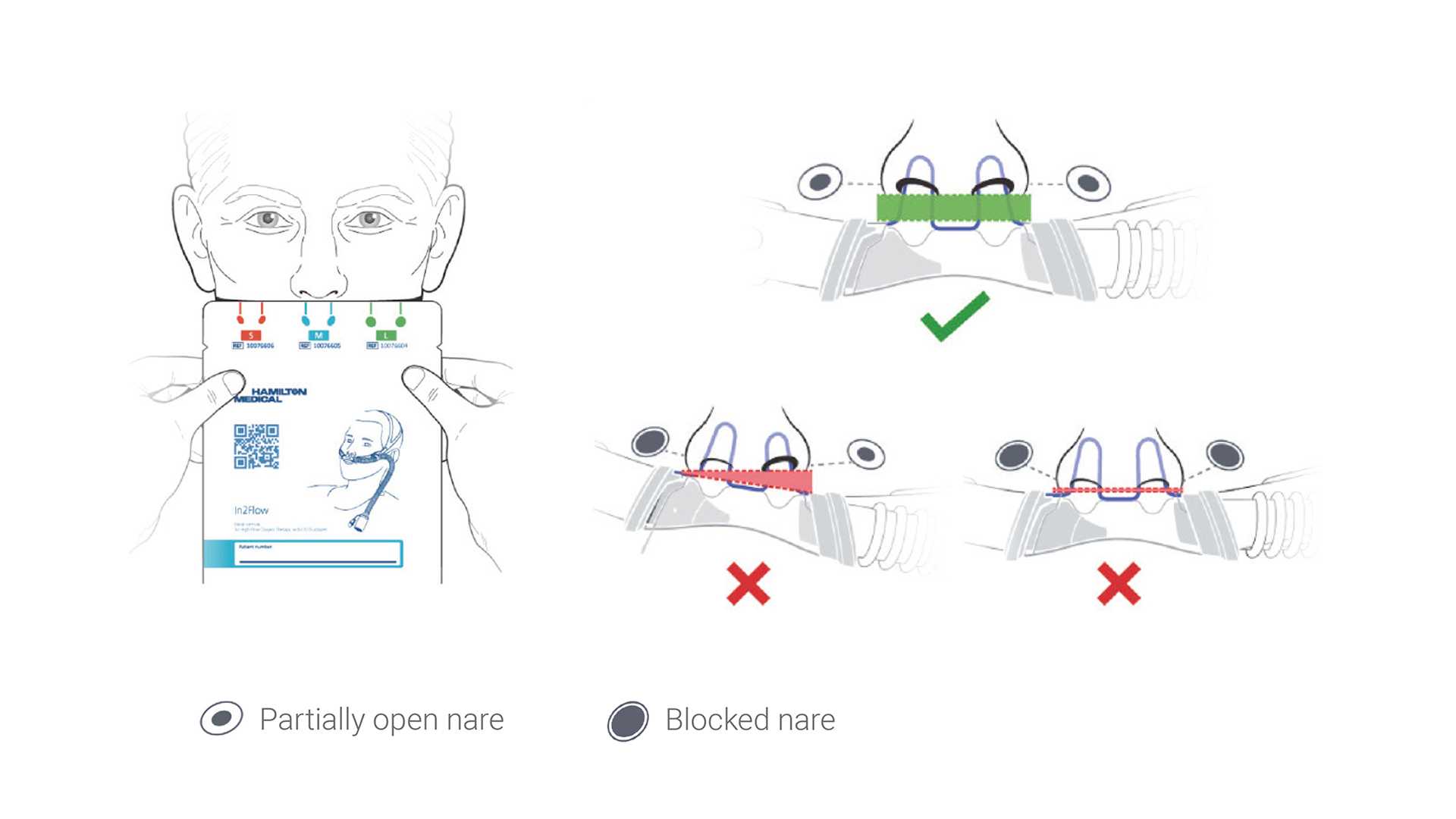
The nasal cannula interface is an essential component for delivery of high flow nasal cannula therapy. In order to maintain an effective flush of CO2, it is important that the cannula does not occlude more than ~50% of the nares.
Good to know: Airway pressure increases progressively with both increasing flow rate and nasal prong‑to‑nares ratio.


Below you can find the recommendations on how to set the flow and oxygen in adult and pediatric patients.
Important: Please note that they are only general recommendations, and every patient should be treated based on their specific medical condition.
(
Flow rates that exceed inspiratory demand can be set in patients under 24 months who tolerate flows of 1 to 2 l/kg/min (up to 20 l/min).
(
| Age | Body weight (kg) | Flow range (l/min) |
| ≤ 1 month | < 4 | 5‑8 |
| 1‑12 months | 4‑10 | 8‑20 |
| 1‑6 years | 10‑20 | 12‑25 |
| 6‑12 years | 20‑40 | 20‑30 |
| 12‑18 years | > 40 | 25‑50 |
The FiO2 is the concentration of oxygen in the gas mixture delivered to the patient. In HFNC, the FiO2 should be set as follows:

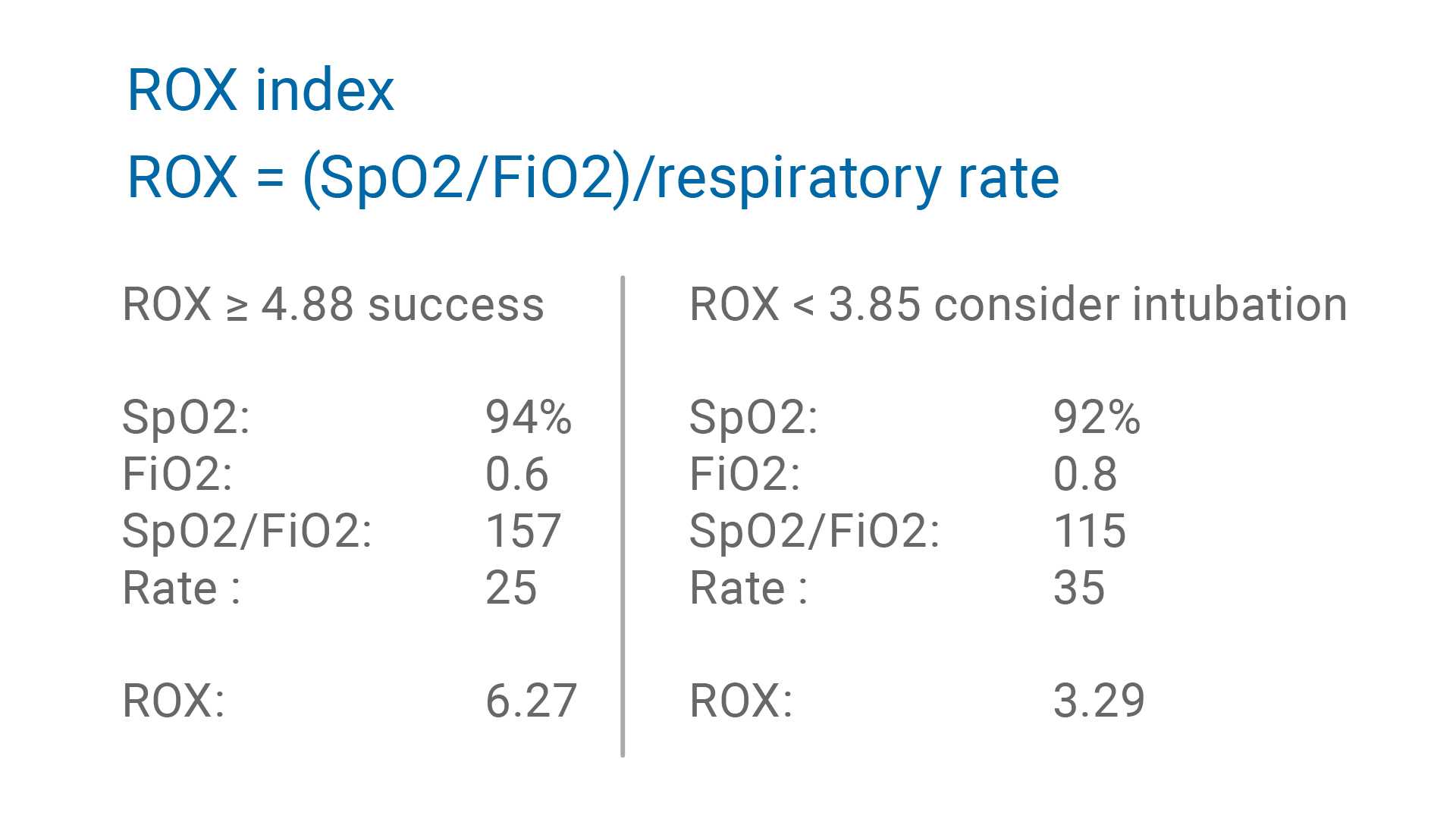
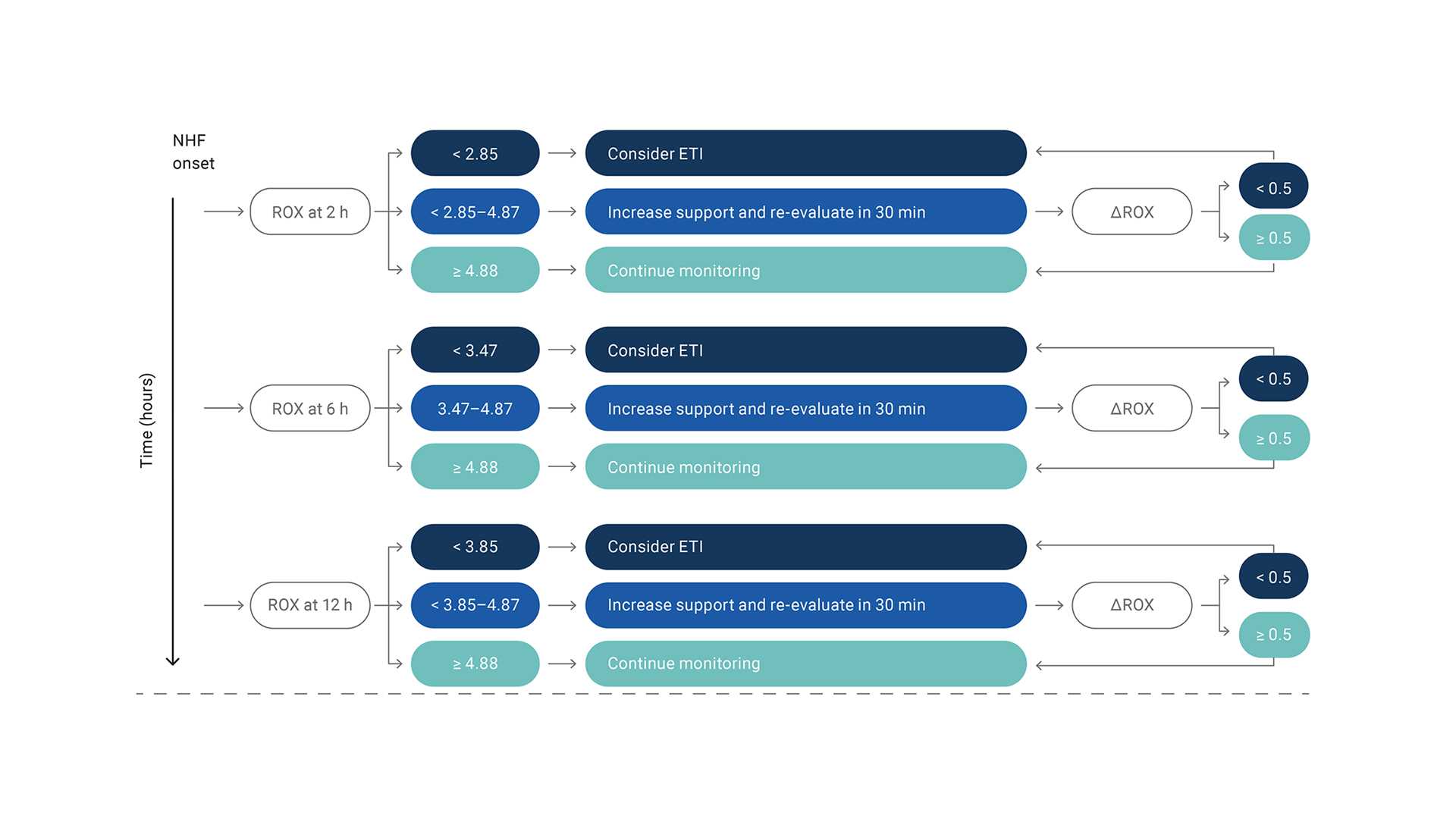
The ROX index is defined as the ratio of oxygen saturation as measured by SpO2/FiO2 to the respiratory rate. In patients with hypoxemic respiratory failure, the ROX index can be used after HFNC therapy has been initiated to help identify those who are at high risk of intubation (
ROX index ≥ 4.88 after two hours of treatment, indicates a high probability that intubation will not be necessary.
ROX index < 3.85 indicates a higher risk of treatment failure.

(

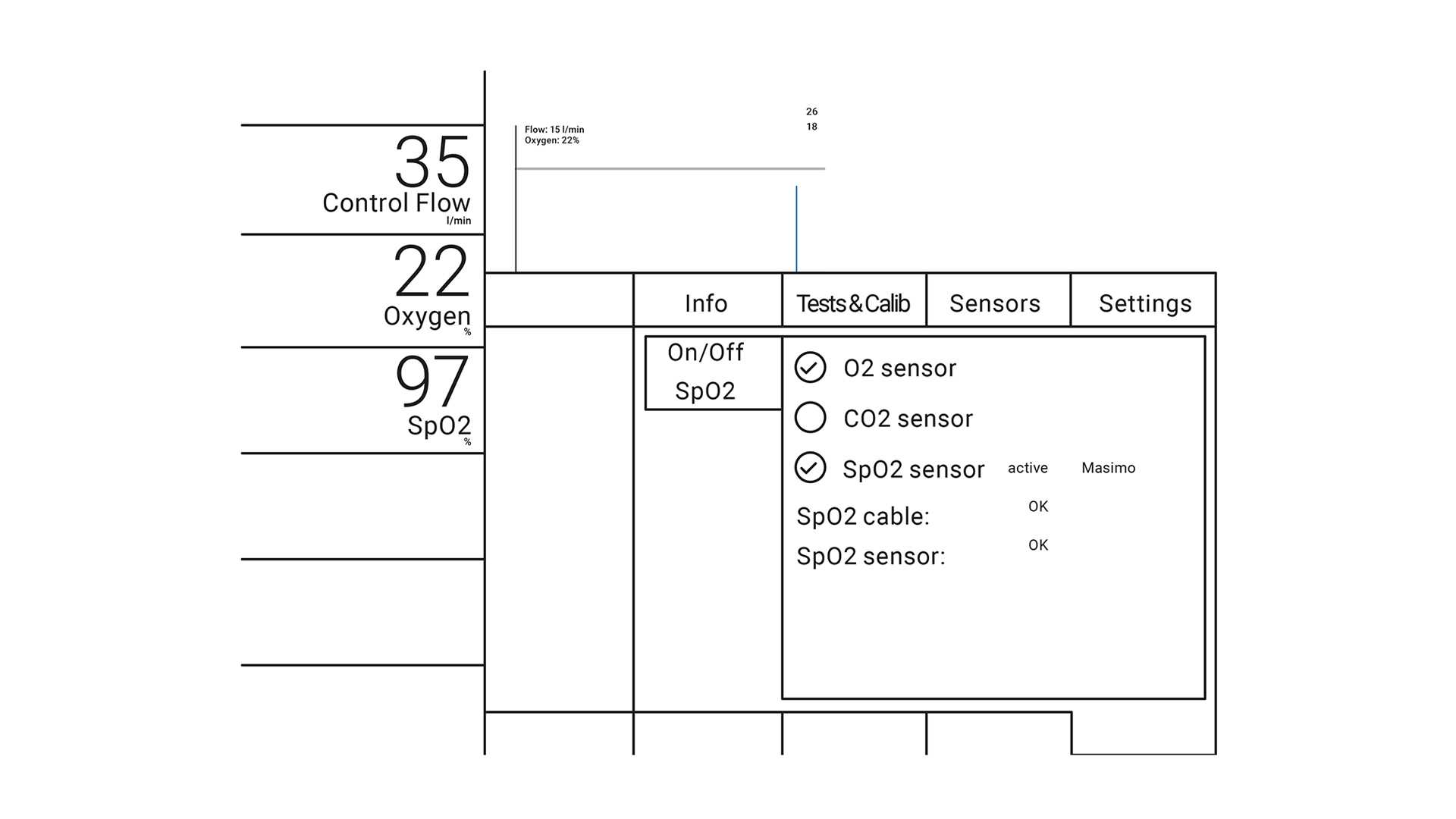
SpO2 is one of the most important parameters to monitor during HFNC. It indicates whether FiO2 needs to be re‑adjusted and is useful during FiO2 titration.
How to use SpO2 (

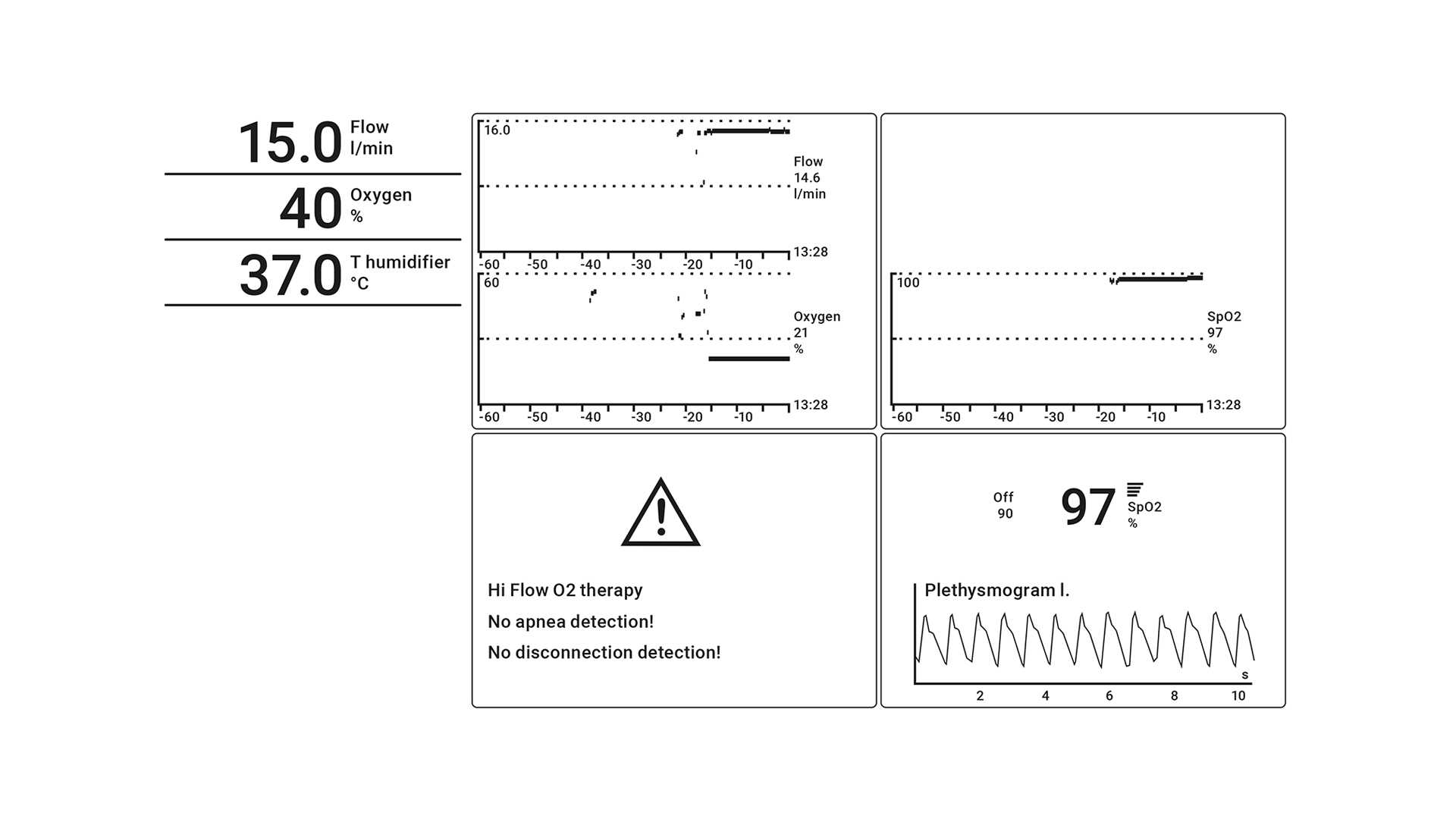
The monitoring shows the values of flow and oxygen over time so you can evaluate the therapy's progress.
How to monitor the progress of the therapy with your Hamilton Medical ventilator:
Trending graphs:

Ventilators from Hamilton Medical offer high flow oxygen therapy as a standard or optional feature, in addition to continuous SpO2 and SpO2/FiO2 measurement (
It is also available on our standalone high flow oxygen therapy device, the HAMILTON‑HF90 (
We also have some exclusive offers for HFNC enthusiasts where something exciting about high flow nasal cannula therapy is waiting you.

Something exciting about high flow nasal cannula therapy is waiting you. Visit the page to learn more.

High flow oxygen therapy combines several physiologic effects.

High‑flow therapy (HFT) is a non‑invasive form of respiratory support that can lower the intubation rate and mortality in patients with acute hypoxemic respiratory failure (AHRF) (1). Driven by concerns about the exposure of healthcare workers, initial recommendations discouraged the use of HFT in COVID‑19 patients (2, 3).

The coronavirus pandemic has stretched many hospitals’ resources to the limit. Patients are requiring respiratory support on an unprecedented scale and a possible ‑ or in some cases very real ‑ shortage of ventilators is forcing institutions to weigh up the risks and benefits of alternative forms of therapy.

Work of breathing (WOB) represents the integral of the product of volume and pressure. It represents the energy associated with a given VT at a given pressure (spontaneous, mechanical, or both).